4. DISEASE MANAGEMENT
4.1. Overactive bladder
4.1.1. Epidemiology, aetiology, pathophysiology
Overactive bladder syndrome is defined by the ICS as “urinary urgency, usually accompanied by frequency and nocturia, with or without UUI, in the absence of UTI or other obvious pathology” [113]. Overactive bladder is a chronic condition that can have debilitating effects on QoL. The hallmark urodynamic feature is DO but the diagnosis of OAB is exclusively based on symptoms.
The EPidemiology of InContinence (EPIC) study [114] was a cross-sectional telephone survey of adults conducted in five countries and demonstrated an overall prevalence of OAB symptoms of 11.8% (10.8% in men and 12.8% in women).
Various theories have been proposed to explain the pathophysiology of OAB, mainly relating to imbalances in inhibitory and excitatory neural pathways to the bladder and the urethra or sensitivity of bladder muscle receptors. However, no definite identifiable causes have been established.
4.1.2. Classification
Overactive bladder is generally classified into wet and dry, based on the presence or absence of associated UI.
4.1.3. Diagnostic evaluation
Evaluation of symptoms of OAB follows the general pathway of evaluation of women with LUTS.
4.1.3.1. Bladder diaries
Diaries are particularly helpful in establishing and quantifying symptoms of frequency, urgency and UI, and may be valuable in assessing change over time or response to treatment. Several observational studies have demonstrated a close correlation between data obtained from bladder diaries and standard symptom evaluation [39-42]. The optimum number of days required for bladder diaries appears to be based on a balance between accuracy and compliance. Diary duration of three to seven days is routinely used in the literature. For further information, please review Section 3.3.
4.1.3.2. Urodynamics
Urodynamics is essential in establishing the presence of DO, but its absence does not preclude diagnosis of OAB, which is based on symptoms alone.
A Cochrane review of seven RCTs showed that use of urodynamic tests increased the likelihood of prescribing drugs or avoiding surgery. However, there was no evidence that this influence on decision-making altered the clinical outcome of treatment [77]. A sub-analysis of an RCT comparing fesoterodine to placebo [85] showed that the urodynamic diagnosis of DO was not predictive of treatment response.
4.1.3.3. Summary of evidence and recommendations regarding OAB diagnosis
Summary of evidence | LE |
Bladder diaries of three to seven days’ duration may be helpful in quantifying symptoms of OAB and assessing response to treatment. | 3 |
Urodynamic diagnosis of DO does not influence treatment outcomes in patients with OAB. | 1a |
Recommendations | Strength rating |
Request that patients complete at least a three-day bladder diary at initial evaluation for overactive bladder (OAB). | Strong |
Do not routinely carry out urodynamics when offering first-line treatment to patients with uncomplicated OAB symptoms. | Strong |
4.1.3.4. Urinary biomarkers
A SR and meta-analysis indicated that uNGF, BDNF to creatinine ratio and uNGF to creatinine ratio were all increased in female OAB patients compared to healthy controls, whereas no difference was found for the PGE2/Cr and ATP/Cr ratios [115]. The current data is inadequate to assess any other potential biomarkers, in the diagnosis or management of OAB in female patients.
4.1.4. Disease management
4.1.4.1. Conservative management
In clinical practice, it has long been the convention that non-surgical therapies are recommended first because they usually carry the lowest risk of harm. While this remains true for non-pharmacological conservative treatments [e.g., pelvic floor muscle training (PFMT)], increasing concerns regarding the adverse events of some pharmacological treatments used to treat OAB (e.g., anticholinergic drugs), particularly regarding cognitive function, have emerged and patients should be fully counselled regarding this potential risk.
4.1.4.1.1. Addressing associated medical co-morbidities
Lower urinary tract symptoms, especially in elderly patients, are associated with multiple co-morbid conditions including:
- cardiac failure;
- chronic renal failure;
- diabetes;
- chronic obstructive pulmonary disease;
- neurological disease;
- general cognitive impairment;
- sleep disturbances, e.g., sleep apnoea;
- depression;
- metabolic syndrome.
If a change in co-morbidity or a new treatment for any associated co-morbidity has been linked to a deterioration in LUTS then this should be reviewed.
One study involving middle-aged women with type 1 diabetes mellitus showed that 10% had UUI. The study showed no correlation between early intensive insulin treatment of type 1 diabetes mellitus vs. conventional insulin treatment and the occurrence of UUI. The same study found no difference in the prevalence of UI in these patients later in their lives [116].
4.1.4.1.2. Adjustment of other medication
Although LUTS are listed as adverse effects of many drugs, this mainly derives from uncontrolled individual patient reports and post-marketing surveillance. Few controlled studies used the occurrence of LUTS as a primary outcome or were powered to assess the occurrence of statistically significant LUTS, or worsening rates against placebo. In most cases, it is therefore not possible to be sure that any drug causes OAB/LUTS.
A structured scoping review failed to identify any studies addressing whether adjustment of specific medications could alter existing symptoms of OAB.
4.1.4.1.2.1. Summary of evidence and recommendations for conservative management of OAB
Summary of evidence | LE |
There is a lack of evidence that improving any associated co-morbid condition improves OAB. | 3 |
There is little evidence that adjustment of specific medications for associated co morbid conditions can alter existing symptoms of OAB. | 3 |
Recommendations | Strength rating |
Take a history of current medication use from all patients with overactive bladder (OAB). | Strong |
Review any new medication associated with the development or worsening of OAB symptoms. | Strong |
4.1.4.1.3. Urinary containment
Urinary containment is important for people with OAB wet when active treatment does not cure the problem, is delayed, or when it is not available or possible. Some individuals may prefer urinary containment rather than active treatment with its associated risks. Containment includes the use of absorbent pads, urinary catheters, external collection devices and intravaginal devices. Detailed literature summaries can be found in the current International Consultation on Urological Diseases (ICUD) monograph [8] and in a European Association of Urology Nurses guidance document [117].
A SR of five RCTs comparing different types of pads found that pads filled with superabsorbent material were better than standard pads but evidence that disposable pads in preventing skin problems, were better than washable pads was inconsistent [118]. A series of three crossover RCTs examined performance of different pad designs for differing populations [119]. For women with light UI, disposable insert pads (within washable pouch pants) were most effective. In adults with moderate/severe UI, disposable pull-up pants were more effective for women.
A Cochrane review summarised three RCTs comparing different types of long-term indwelling catheters and found no evidence that one catheter material or type of catheter was superior to another [120]. A SR of non-randomised studies found no differences in UTI outcome or UUT changes between use of suprapubic or urethral catheter drainage; however, patients with suprapubic catheters were less likely to have urethral complications [121].
Catheter-related bladder discomfort may be significant in women. Anticholinergics have been proposed to prevent or reduce this issue, but most of the evidence comes from clinical trials in the postoperative period, and the results are conflicting [122-125]. One retrospective study including 40 women (most of them neurogenic) with long-term bladder catheters found intravesical botulinum toxin injections helped to prevent bladder pain and discomfort and catheter bypass/leakage. Patients reported an improvement in QoL and a significant 83% reduction in urine leakage [126].
A Cochrane review summarising five trials comparing bladder washout policies in adults with indwelling urinary catheters found inconsistent evidence of benefit [127].
A Cochrane review summarising eight trials of whether antibiotic prophylaxis was beneficial for adults using clean intermittent self-catheterisation (CISC) or indwelling catheterisation found it reduced the incidence of symptomatic UTI but possible harms were not assessed [128]. A multicentre RCT from the UK involving patients practising CISC reported that prophylaxis reduced UTI incidence and was well-tolerated, but development of antibiotic resistance was a concern [129].
4.1.4.1.3.1. Summary of evidence and recommendations for urinary containment
Summary of evidence | LE |
Pads are effective in containing urine. | 1b |
Antibiotic prophylaxis may help reduce incidence of UTI in patients who have an indwelling catheter or use CISC, but at the cost of increasing antimicrobial resistance. | 1a |
Recommendations | Strength rating |
Ensure that women with overactive bladder (OAB) and/or their carers are informed regarding available treatment options before deciding on urinary containment alone. | Strong |
Offer incontinence pads and/or containment devices for management of OAB wet, either for temporary symptom control or when other treatments are not planned. | Strong |
Offer prophylactic antibiotics to patients on clean intermittent self-catheterisation or on indwelling catheter with recurrent urinary tract infection only after discussion regarding the risk of increasing antimicrobial resistance. | Strong |
4.1.4.1.4. Lifestyle interventions
Examples of lifestyle factors that may be associated with UI include obesity, smoking, level of physical activity, regulation of bowel habit, and fluid intake. Modification of these factors may improve symptoms of OAB.
4.1.4.1.4.1. Caffeine intake
A scoping review of fourteen interventional and twelve observational studies reported that reduction in caffeine intake may reduce symptoms of urgency, but the certainty of evidence was low, with significant heterogeneity in study populations [130].
4.1.4.1.4.2. Fluid intake
Modification of fluid intake, particularly restriction, is a strategy commonly used by people with OAB. Any advice on fluid intake given by health care practitioners (HCPs) should be based on 24-hour fluid intake and urine output measurements as retrieved from the bladder diary. From a general health point of view, it should be advised that fluid intake should be sufficient to avoid thirst and that an abnormally low or high 24-hour urine output should be investigated. The few published RCTs involving women provide inconsistent evidence [131-133]. In most studies, the instructions for fluid intake were individualised and it was difficult to assess participant adherence. An RCT showed that a reduction in fluid intake by 25% improved symptoms in patients with OAB but did not improve UI [133]. Personalised fluid advice compared to generic advice made no difference to continence outcomes in people receiving anticholinergics for OAB, according to an RCT comparing drug therapy alone to drug therapy with behavioural advice [134]. Patients should be warned of the potential consequences of fluid restriction such as worsening of constipation or development of UTI.
4.1.4.1.4.3. Weight loss
Being overweight or obese has been identified as a risk factor for LUTS in epidemiological studies [135,136]. There is evidence that the prevalence of both UUI and SUI increases proportionately with body mass
index (BMI) [137]. However, the evidence base largely relates to obesity and SUI rather than UUI and OAB. Therefore, no definite inference can be drawn between obesity and the prevalence of OAB.
4.1.4.1.4.4. Smoking cessation
Smoking cessation is a general public health measure and has been shown to be weakly associated with improving urgency, frequency, and UI [138,139]. The effect of smoking cessation on LUTS was described as uncertain in a health technology assessment review [140].
4.1.4.1.4.5. Summary of evidence and recommendations for lifestyle interventions
Summary of evidence | LE |
Reduction of caffeine intake may reduce symptoms of frequency and urgency. | 2 |
Reduction in fluid intake by 25% may help improve symptoms of OAB but not UI. | 1b |
Personalised fluid intake advice when added to pharmacotherapy provides no additional benefit in patients with OAB. | 2 |
Obesity is a risk factor for UI in women, but the relationship to other OAB symptoms remains unclear. | 1b |
There is weak evidence that smoking cessation improves symptoms of OAB. | 3 |
Recommendations | Strength rating |
Advise adults with OAB that reducing caffeine intake may improve symptoms of urgency and frequency, but not incontinence. | Strong |
Review type and amount of fluid intake in patients with OAB. | Weak |
Encourage overweight and obese adults with overactive bladder (OAB)/urinary incontinence to lose weight and maintain weight loss. | Strong |
Provide smoking cessation strategies to patients with OAB who smoke. | Strong |
4.1.4.1.5. Behavioural and physical therapies
Behavioural and physical therapies are often introduced as part of a package of care including lifestyle changes and patient education.
4.1.4.1.5.1. Prompted voiding and timed voiding
The term ‘prompted voiding’ implies that carers, rather than the patient, initiate the patient going to void with the aim of preventing or reducing UI. This applies largely to an assisted care setting. A SR (nine RCTs including mostly women with UI), comparing prompted voiding to standard care, suggested evidence of short-term benefit for management of UI [141].
Timed voiding is defined as fixed, predetermined, time intervals between voids and is applicable for those with or without cognitive impairment. A Cochrane review of timed voiding included four RCTs and found inconsistent improvement in continence compared with standard care in cognitively impaired adults [142].
4.1.4.1.5.2. Bladder training
Bladder training (BT) is a programme of patient education along with a scheduled voiding regimen with gradually increasing intervals. Specific goals are to correct faulty patterns of frequent urination, improve control over bladder urgency, prolong voiding intervals, increase bladder capacity, reduce incontinent episodes and restore patient confidence in controlling bladder function. The ideal form or intensity of a BT programme for OAB/UI is unclear.
A comparison of anticholinergic treatment with BT in one Cochrane review with seven RCTs showed inconsistent results in terms of cure rates but reported significantly more patients improved with anticholinergics [143]. The same review showed that the addition of anticholinergics to BT as part of behavioural modification resulted in more subjective improvement but no difference in objective outcomes.
Cognitive behavioural therapy involves the analysis of or change to a thought process related to the sensation of urgency or employment of a specified thought process during an episode of urgency. This includes mental distraction (the most common), relaxation and mindfulness practices. A SR on cognitive components of behavioural therapies for OAB concluded that they were neither well described nor rationalized. Behavioural therapy that includes cognitive component shows promise for OAB treatment, but its relative importance has not been well evaluated nor rigorously studied [144].
Another SR including 12 studies on the effect of cognitive behavioural therapy on women with UUI showed high level of evidence of its effectiveness on improving symptom severity and moderate level of evidence on QoL, psychological symptoms and patient satisfaction when compared with placebo. However, results were inconsistent with some studies showing no difference in objective parameters such as bladder capacity [145].
4.1.4.1.5.3. Pelvic floor muscle training
Pelvic floor muscle contraction can lead to simultaneous inhibition of urgency, detrusor contraction and incontinence [146]. Intensive and regular strength training of the PFMs over time increases both PFM contraction strength and endurance, and changes the morphology of the pelvic floor, which may yield more effective inhibition of the detrusor and help to stabilize the proximal urethra and improve urethral function. There is a lack of basic and mechanistic studies to confirm that change in pelvic floor morphology improves OAB symptoms.
A SR of eleven RCTs [147] including women with OAB compared the efficacy of PFMT vs. inactive control, usual care, other lifestyle modification or other intervention. Pelvic floor muscle training significantly reduced OAB symptoms (frequency and UUI) in five RCTs, while the remaining six reported no significant difference. Significant heterogeneity in protocols and outcomes was noted.
4.1.4.1.5.4. Electrical stimulation
The methods of delivery of electrical stimulation (ES) vary considerably. Electrical stimulation of the PFM can also be combined with other forms of conservative therapy, e.g., PFMT with and without biofeedback. Electrical stimulation is often used to assist women who cannot initiate contractions to identify their PFMs and in patients with OAB and UUI with the aim of inhibiting detrusor contraction. There is, however, a lack of basic and mechanistic studies to confirm this theory.
A SR of the effect of ES included 63 trials with 4,224 adults with OAB symptoms [148]. Moderate-quality evidence suggests that ES is more likely to improve OAB symptoms compared to sham control, no treatment, PFMT, and drug treatment. It was unclear if ES was more effective than placebo/sham for UUI. Insufficient or very low-quality evidence was available to determine the difference in the adverse event rates between ES and placebo/sham and the other active treatments.
A SR of nine studies compared the effects different techniques of electrical stimulation. Pooled analysis of three trials showed no difference between intravaginal stimulation and transcutaneous posterior tibial nerve stimulation (T-PTNS) in terms of urinary frequency, nocturia and QoL scores [149]. In the same review, pooled results from two studies which T-PTNS was compared with posterior tibial nerve stimulation (PTNS) showed no difference in urinary urgency, frequency and QoL scores [149].
4.1.4.1.5.4.1.Posterior tibial nerve stimulation
Electrical stimulation of the posterior tibial nerve delivers electrical stimuli to the sacral micturition centre via the S2–S4 nerve roots. Stimulation is percutaneous with a fine (34-G) needle, inserted just above the medial aspect of the ankle (P-PTNS). Transcutaneous stimulation is also available that delivers stimulation via surface electrodes that do not penetrate the skin. The optimal treatment schedule has not been determined, with daily and weekly regimens described [150].
A SR identified five RCTs (408 women) that compared PTNS with antimuscarinics. The PTNS techniques were significantly more effective than antimuscarinics in the reduction of UUI episodes with no significant difference in the reduction of overall symptoms score, frequency episodes or urgency episodes [11].
A SR of three studies comparing PTNS monotherapy with PTNS plus antimuscarinics, showed that the combination therapy added no statistically significant difference to PTNS monotherapy in the reduction of mean symptoms score, frequency episodes, nocturia episodes, or UUI episodes [11].
4.1.4.1.5.4.2.Percutaneous posterior tibial nerve stimulation
The reviewed studies included a SR, two twelve-week RCTs of P-PTNS compared with sham treatment [151-153], one RCT comparing PTNS to tolterodine, and a three-year extension trial utilising a maintenance protocol in patients with OAB [154,155]. The results of studies of PTNS in women with OAB consistently showed significant and sustained improvement in symptoms from baseline, with similar improvement compared to treatment with tolterodine.
4.1.4.1.5.4.3.Transcutaneous posterior tibial nerve stimulation
A SR of thirteen trials (ten RCTs and three cohort studies) compared the efficacy of T-PTNS (duration four to twelve weeks) with sham treatment, anticholinergics, and exercise in treatment of adults with OAB symptoms [156]. Of note, the populations were adult women and men, and some studies included patients with neurogenic OAB. Meta-analysis was possible in two RCTs comparing T-PTNS with sham treatment and revealed mean reduction in total International Consultation on Incontinence modular questionnaire (ICIQ) Urinary Incontinence Short Form (ICIQ-UI-SF) associated with T-PTNS of −3.79 points.
A small RCT compared T-PTNS plus standard treatment (PFMT and BT) with PFMT and BT alone in older women [157]. Women in the T-TPNS group were more likely to achieve improvement.
A small RCT compared BT alone, BT plus P-PTNS and BT plus T-PTNS in women with idiopathic OAB. Both P-PTNS and T-PTNS were more effective than BT alone. These two tibial nerve stimulation methods had similar clinical efficacy but with slight differences: T-PTNS had shorter preparation time, less discomfort level and higher patient satisfaction than P-PTNS [158].
4.1.4.1.5.5. Acupuncture
A SR with meta-analysis of ten RCTs including 794 patients (590 women) reported that acupuncture might have an effect in reducing OAB symptoms compared to sham treatment [159]. The studies were of low quality and compared electro-acupuncture vs. sham acupuncture, or electro-acupuncture plus tolterodine vs. tolterodine alone.
4.1.4.1.5.6. Summary of evidence and recommendations for behavioural and physical therapies
Summary of evidence | LE |
Prompted voiding, either alone or as part of a behavioural modification programme, improves continence in elderly, care-dependent, people in the short-term. | 1b |
Bladder training is effective for improvement of UUI in women, but efficacy appears to be lower than that of pharmacotherapy. | 1b |
Pelvic floor muscle training may improve symptoms of frequency of OAB in women. | 1b |
Electrical stimulation may improve symptoms of OAB in some women, but the type and mode of delivery of ES remains variable and poorly standardised. | 1a |
Posterior tibial nerve stimulation is more effective than antimuscarinics in reducing UUI episodes but with no difference in improving other OAB symptoms. | 1a |
A maintenance programme of P-PTNS has been shown to be effective for up to 3 years. | 2a |
Transcutaneous-PTNS appears to be effective in reducing OAB symptom compared to sham treatment. | 1a |
Transcutaneous -PTNS is not inferior to percutaneous -PTNS with regard to improvement in urinary urgency, frequency, and QoL scores. | 1a |
Recommendations | Strength rating |
Offer prompted voiding to adults with overactive bladder (OAB) who are cognitively impaired. | Strong |
Offer bladder training as a first-line therapy to adults with OAB/urge urinary incontinence (UUI). | Strong |
Ensure that pelvic floor muscle training programmes are as intensive as possible. | Strong |
Consider posterior tibial nerve stimulation as an option for symptomatic improvement of OAB/UUI. | Strong |
4.1.4.2. Pharmacological management
4.1.4.2.1. Anticholinergic drugs
Anticholinergic (antimuscarinic) drugs are currently the mainstay of treatment for OAB. Different agents vary in their pharmacological profiles, such as muscarinic receptor affinity and other modes of action and in their pharmacokinetic properties, such as lipid solubility and half-life.
The Panel SR identified twelve studies (11,179 women) comparing antimuscarinics with placebo. Antimuscarinics were significantly more effective than placebo in improving mean symptom score on OABQ, reducing daily frequency episodes, reducing daily urgency episodes and UUI episodes, and increasing bladder functional capacity [11].
The SR established that antimuscarinics caused significantly higher adverse events than placebo including dry mouth, cognitive impairment, UTI and constipation [11].
Immediate-release (IR) anticholinergic preparations provide maximum dosage flexibility, including an off-label on-demand use. Immediate-release drugs have a greater risk of adverse effects than extended release (ER) formulations because of differing pharmacokinetics. A transdermal delivery system and gel developed for oxybutynin provide alternative formulations. On balance, IR formulations tend to be associated with more adverse effects compared to ER formulations [160].
A network meta-analysis of 128 RCTs including both genders comparing anticholinergics with placebo or other anticholinergics revealed that all anticholinergics, except imidafenacin, showed reasonable cure or improvement rates for OAB symptoms in both sexes [161]. Differences across the drugs in terms of alteration in symptoms were small.
Cure of UUI is deemed to be the most important outcome measure. Table 1 shows a summary of the findings from a SR of RCTs including only women [162]. All agents showed superiority compared to placebo, but the absolute size of the effect was small.
Table 1: Summary of cure and discontinuation rates of anticholinergic drugs from RCTs
Drug | No. of studies | No. of patients | RR (95% CI) (of curing UI) | NNT (95% CI) (to achieve one cure of UI) |
Cure of incontinence | ||||
Fesoterodine | 2 | 2,465 | 1.3 (1.1–1.5) | 8 (5–17) |
Oxybutynin (includes IR) | 4 | 992 | 1.7 (1.3–2.1) | 9 (6–16) |
Propiverine (includes IR) | 2 | 691 | 1.4 (1.2–1.7) | 6 (4–12) |
Solifenacin | 5 | 304 | 1.5 (1.4–1.6) | 9 (6–17) |
Tolterodine (includes IR) | 4 | 3,404 | 1.2 (1.1–1.4) | 12 (8–25) |
Trospium (includes IR) | 4 | 2,677 | 1.7 (1.5–2.0) | 9 (7–12) |
Discontinuation due to adverse events | ||||
RR (95% CI) (of discontinuation) | NNT (95% CI) (for one discontinuation) | |||
Darifenacin | 7 | 3,138 | 1.2 (0.8–1.8) | |
Fesoterodine | 4 | 4,433 | 2.0 (1.3–3.1) | 33 (18–102) |
Oxybutynin (includes IR) | 5 | 1,483 | 1.7 (1.1–2.5) | 16 (8–86) |
Propiverine (includes IR) | 2 | 1,401 | 2.6 (1.4–5) | 29 (16–77) |
Solifenacin | 7 | 9,080 | 1.3 (1.1–1.7) | 78 (39–823) |
Tolterodine (includes IR) | 10 | 4,466 | 1.0 (0.6–1.7) | |
Trospium (includes IR) | 6 | 3,936 | 1.5 (1.1–1.9) | 56 (30–228) |
CI = confidence interval; IR = immediate release; NNT = number to treat; RR = relative risk;UI = urinary incontinence.
The cure rates for darifenacin were not included in the US Agency for Healthcare Research and Quality (AHRQ) review. Continence rates were 29–33% for darifenacin compared to 17–18% for placebo [163]. Transdermal oxybutynin showed a significant improvement compared with placebo and other oral formulations in the number of incontinence episodes and micturitions per day but cure of UI was not reported as an outcome [163]. Oxybutynin topical gel was superior to placebo for improvement of UUI, with a higher proportion of participants being cured [163,164].
4.1.4.2.1.1. Comparison of different anticholinergic agents
Head-to-head comparison trials of the efficacy and adverse effects of different anticholinergic agents are of interest for decision-making.
Both a network meta-analysis and a SR revealed no superior anticholinergic preparation for cure or improvement [161,165]. There were no clinically significant differences between anticholinergics for voiding and UI outcomes. No single anticholinergic agent improved QoL more than another [165].
Conflicting results were reported from another network meta-analysis of 53 RCTs that compared the efficacy and tolerability of solifenacin 5 mg/day with other oral anticholinergics in the treatment of adults with OAB symptoms [166]. Solifenacin 5 mg/day was significantly more effective than tolterodine 4 mg/day for reducing UUI episodes, but significantly less effective than solifenacin 10 mg/day for reducing micturition episodes. Solifenacin 5 mg/day showed significantly lower risk of dry mouth compared with other anticholinergics but no significant differences for the risk of blurred vision or constipation.
A further network meta-analysis with 128 RCTs including both genders showed that all anticholinergics were worse than placebo in terms of dry mouth with transdermal oxybutynin having the smallest difference [161].
Dry mouth is the most prevalent reported adverse effect. Extended-release formulations are associated with lower rates of dry mouth than IR preparations [165,167]. Oxybutynin IR shows higher rates of dry mouth than tolterodine IR and trospium IR but lower rates of dry mouth than darifenacin, 15 mg daily [165,167]. Overall, oxybutynin ER causes higher rates of dry mouth than tolterodine ER does, although the incidence of moderate or severe dry mouth is similar. Transdermal oxybutynin has a lower rate of dry mouth than oxybutynin IR and tolterodine ER but an overall higher rate of withdrawal due to adverse skin reactions [165]. Solifenacin 10 mg daily has higher rates of dry mouth than tolterodine ER [165]. Fesoterodine 8 mg daily has a higher rate of dry mouth than tolterodine 4 mg daily [168-170]. Similar discontinuation rates have been observed, irrespective of differences in the occurrence of dry mouth.
It is notable that nearly all the primary studies in this category were industry sponsored. In general, these studies have been designed to achieve regulatory approval. Upward dose titration is often included in the protocol for the experimental arm but not for the comparator arm. They have short treatment durations (twelve weeks) and a primary outcome of a change in OAB symptoms rather than a cure of, or an improvement in, UUI, which were generally analysed as secondary outcomes. The clinical utility of these trials in real-life practice is therefore debatable. Most trials were of low or moderate quality [165].
4.1.4.2.1.2. Anticholinergic drugs versus conservative treatment
More than 100 RCTs and high-quality reviews are available detailing relative efficacy of anticholinergic drugs and conservative treatment strategies [143,165,171-174]. Most of these were independent studies. The main focus of the reviews was to compare the different drugs used to treat UUI. A U.S. health technology assessment [172] found that the vast majority of trials were of a low or moderate quality.
4.1.4.2.1.2.1. Anticholinergic drugs in combination with other conservative treatment versus anticholinergic drugs alone
The combination of BT and solifenacin in female patients with OAB confers no additional benefit in terms of continence compared with solifenacin monotherapy [175]. A recent Cochrane review on the benefit of adding PFMT to other active treatments of UI in women showed insufficient evidence of any benefit in adding PFMT to drug treatment [176].
One SR identified thirteen RCTs comparing outcomes of antimuscarinic mono-therapy with combinations of antimuscarinics plus adjunct treatments including topical oestrogen, pregabalin, Stroller neurostimulation (SANS), PFMT, and behavioural therapy. Antimuscarinics alone were less effective than a combination of antimuscarinics plus another treatment modality in reducing urgency episodes, UUI episodes, frequency and nocturia episodes and in improving the mean symptoms score but no significant differences were found in rates of dry mouth, constipation or voiding dysfunction [11].
4.1.4.2.1.3. Anticholinergic drugs: adherence and persistence
Most studies on anticholinergic medication are short term (twelve weeks). Adherence in clinical trials is considered to be higher than in clinical practice [177]. Discontinuation rates were high for tolterodine at twelve months, and particularly high (68–95%) for oxybutynin. Two open-label extensions of RCTs of fesoterodine
8 mg showed adherence rates at two years of 49–84% [178,179].
A longitudinal disease analyser database study has indicated an increasing discontinuation rate, following treatment with anticholinergics, from 74.8% at one year to 87% at three years [180].
Several of the RCTs tried to identify the factors associated with low/lower adherence or persistence of anticholinergics. These were identified as:
- low level of efficacy (41.3%);
- adverse events (22.4%);
- cost (18.7%), although higher adherence rates were observed when drugs were provided at no cost to patients [181].
Other factors associated with poor adherence included:
- immediate release formulations (lower persistence compared with ER formulations);
- age (lower persistence among younger adults);
- unrealistic expectations of treatment;
- gender distribution (better adherence/persistence in female patients);
- ethnic group (African–Americans and other ethnic minorities are more likely to discontinue or switch treatment).
4.1.4.2.1.4. Summary of evidence and recommendations for anticholinergic drugs
Summary of evidence | LE |
Anticholinergic drugs are effective in improving OAB symptoms, decreasing UUI episodes, decreasing daily urgency and frequency episodes and increasing mean voided volumes, compared with placebo. | 1a |
Anticholinergic drugs caused higher adverse events than placebo including dry mouth, cognitive impairment, and constipation. | 1a |
Once daily (ER) formulations are associated with lower rates of adverse events compared to IR preparations. | 1b |
Transdermal oxybutynin is associated with lower rates of dry mouth than oral anticholinergic drugs but has a higher rate of withdrawal due to skin reactions. | 1b |
Higher doses of anticholinergic drugs are more effective to improve OAB symptoms but exhibit a higher risk of adverse effects. | 1a |
No anticholinergic drug is clearly superior to another for cure or improvement of OAB/UUI. | 1a |
The combination of antimuscarinics plus another treatment modality was more effective than antimuscarinics alone in improving OAB. | 1a |
Adherence to anticholinergic treatment is low and decreases over time because of lack of efficacy, adverse events and/or cost. | 2a |
Most patients will stop anticholinergic agents within the first three months. | 2a |
Recommendations | Strength rating |
Offer anticholinergic drugs to woman with overactive bladder (OAB) who fail conservative treatment. | Strong |
Consider extended-release formulations of anticholinergic drugs whenever possible. | Strong |
If an anticholinergic treatment proves ineffective, consider dose escalation, offering an alternative anticholinergic formulation, or the use of mirabegron (alone or in combination with an anticholinergic). | Strong |
Encourage early review (of efficacy and adverse effects) of patients on anticholinergic medication for OAB. | Strong |
4.1.4.2.2. Beta-3 Agonists
Beta-3 adrenoceptors are the predominant beta receptors expressed on detrusor smooth muscle cells and their stimulation is thought to induce detrusor relaxation. Mirabegron was the first clinically available beta-3 agonist. Vibegron is another beta-3 agonist commercially available in some countries.
Mirabegron has undergone evaluation in industry-sponsored phase II and III trials [182-185]. Three SRs assessing the clinical effectiveness of mirabegron [182,183,186] reported that mirabegron at doses of 25, 50 and 100 mg results in significantly greater reduction in UI episodes, urgency episodes and micturition frequency than placebo, with no difference in the rate of common adverse events [183]. The dry rates in most of these trials are 35–40% for placebo and 43–50% for mirabegron. In all trials the significant differences were consistent only for improvement but not for cure of UI. Similar improvements in the frequency of UI episodes and micturition frequency were found whether or not patients had previously tried anticholinergic agents.
The most common adverse events in the mirabegron groups were hypertension (7.3%), nasopharyngitis (3.4%) and UTI (3%), with the overall rate similar to that with placebo [182,185,187].
A SR with meta-analysis of data pooled from three RCTs comparing vibegron (75 mg or 100 mg) with placebo in 2,120 patients with OAB revealed significant improvement of urgency episodes and UUI episodes and mean voided volume associated with vibegron [188]. The review also reported that vibegron showed a favourable safety profile. Another SR that included three high-quality RCTs compared vibegron with anticholinergic monotherapy (imidafenacin and tolterodine) concluding similar efficacy in terms of improvements in mean number of micturitions, urgency and UUI, but with less dry mouth [189].
4.1.4.2.2.1. Beta-3 agonists versus anticholinergics
One SR [190] assessed the outcomes of mirabegron in women with OAB. It included seven RCTs, three non-randomised comparative studies and eleven observational studies. The review reported no statistical difference between mirabegron and anticholinergics in decreasing OAB symptoms on voiding diaries and symptom questionnaires on short-term follow-up (up to twelve weeks). However, at one year follow-up, there was a statistically significant decrease in OAB symptoms in favour of mirabegron.
Another SR identified four studies on 371 women that compared beta-3 agonists with antimuscarinics. Pooled analysis for the studies showed that beta-3 agonists were significantly more effective than antimuscarinics in reducing nocturia episodes. No significant differences were found between antimuscarinics and beta-3 agonists in reduction of mean symptoms score, urgency episodes, frequency episodes, UUI episodes, or voided volumes [11].
Antimuscarinics caused higher rates of dry mouth than beta-3 agonists, but no significant difference was found in constipation rates [11].
Post hoc analyses of RCTs showed that clinical improvement in OAB severity translates into improvement in HRQoL and efficacy is maintained in patients with more severe UI [191,192]. No risk of QTc prolongation [193] and no raised intraocular pressure [194] were observed up to the 100 mg dose; however, patients with uncontrolled hypertension or cardiac arrhythmia were excluded from these trials. There is no significant difference in the rate of adverse effects at different doses of mirabegron [187].
Equivalent adherence was observed for tolterodine and mirabegron at twelve months (5.5% and 3.6%), although the incidence of dry mouth was significantly higher in the tolterodine group [187]. In mirabegron-treated patients, improvement in objective outcome measures correlates directly with clinically relevant PROMs (Overactive Bladder questionnaire and Patient Perception of Bladder Condition) [191,195]. Data from a large Canadian Private Drug Plan database suggest a higher adherence rate for mirabegron compared to anticholinergics [196].
An RCT in patients who had inadequate response to solifenacin monotherapy 5 mg demonstrated that combination treatment with mirabegron 50 mg had a higher chance of achieving clinically meaningful improvement in UI as compared to dose escalation of solifenacin [197].
4.1.4.2.2.2. Summary of evidence and recommendation for Beta-3 agonists
Summary of evidence | LE |
Mirabegron and vibegron are better than placebo for improvement of OAB/UUI symptoms. | 1a |
Adverse event rates with mirabegron and vibegron are similar to those of placebo. | 1a |
Beta-3 agonists are as effective as antimuscarinics in the management of OAB but with lower dry mouth rates. | 1a |
Patients inadequately treated with solifenacin 5 mg may benefit more from the addition of mirabegron rather than dose escalation of solifenacin. | 1b |
Recommendations | Strength rating |
Offer beta-3 agonists as an alternative to anticholinergics to women with OAB who fail conservative treatment. | Strong |
Offer mirabegron as an additional therapy in patients who are inadequately treated with solifenacin 5 mg. | Weak |
4.1.4.2.3. Anticholinergics and beta-3 agonists: elderly patients and cognition
Systematic reviews have included sections on the efficacy and safety of anticholinergics in elderly patients [163,165] but an older SR found inconclusive evidence of the impact of anticholinergics on cognition [198].
Two more recent longitudinal cohort studies in patients using anticholinergic drugs showed deterioration in cognitive function, alteration in central nervous system metabolism and an association with brain atrophy [199,200]. As most of the study periods are short (four to twelve weeks), the long-term impact of anticholinergic agents specifically approved for OAB treatment on specific patient cohorts are poorly understood [201-204].
- Oxybutynin: There is evidence that oxybutynin IR may cause/worsen cognitive dysfunction in adults [201,203,205,206]. Whilst short-term trials showed no effect on recent memory or other cognitive functions [206], prospective studies showed cumulative cognitive deterioration associated with prolonged use (mean follow-up, 7.3 years) of anticholinergic medication including oxybutynin [199]. Another prospective cohort study including 376 nursing home residents aged 65 and older taking oxybutynin and tolterodine showed a decline in activity of daily living after a median follow-up of 141 days, in spite of concomitant treatment with cholinesterase inhibitors [207].
- Solifenacin: One pooled analysis [208] showed that solifenacin did not increase cognitive impairment in elderly patients. No age-related differences in the pharmacokinetics of solifenacin in different age groups were found, although more frequent adverse events in patients aged > 80 years were observed. No cognitive effect on healthy elderly volunteers was shown [209]. In a sub-analysis of a large trial, solifenacin 5–10 mg improved symptoms and QoL in people aged > 75 years who had not responded to tolterodine [210]. In patients with mild cognitive impairment, aged > 65 years, solifenacin showed no difference in efficacy between age groups and a lower incidence of most adverse effects compared to oxybutynin IR [206,211].
- Tolterodine: No change in efficacy or adverse effects related to age has been reported, although a higher discontinuation rate was found for both tolterodine and placebo in elderly patients [201]. Two RCTs in elderly patients found similar efficacy and adverse effect profile to those in younger patients [212-215]. Post hoc analysis has shown little effect on cognition. One non-randomised comparison showed lower rates of depression in elderly participants treated with tolterodine ER compared to oxybutynin IR [216]. Duration of the RCTs was short (twelve weeks).
- Darifenacin: Two RCTs in the elderly population (one in patients with UUI and the other in volunteers) concluded that, compared with placebo, darifenacin was effective with no risk of cognitive change, measured as memory scanning tests [217,218]. Another study on darifenacin and oxybutynin ER in elderly people concluded that the two agents had similar efficacy, but that cognitive function was more often affected in the oxybutynin ER arm [203].
- Trospium chloride: Trospium does not appear to cross the blood–brain barrier in healthy individuals due to its molecular characteristics (quaternary amine structure and hydrophilic properties). Two studies in healthy volunteers using electroencephalography showed no effect from trospium, while tolterodine caused occasional changes and oxybutynin caused consistent changes [219,220]. No evidence as to the comparative efficacy and adverse effect profiles of trospium in different age groups are available. However, there is some evidence that trospium does not impair cognitive function in Alzheimer’s disease patients if combined with cholinesterase inhibitors over a six month period [204], or in non-cognitively impaired patients over shorter periods (twelve weeks) [221] and that it is effective compared to placebo in the elderly [222].
- Fesoterodine: Pooled analyses of the RCTs of fesoterodine confirmed the efficacy of 8 mg but not 4 mg dose in patients aged > 75 years [178]. Adherence was lower in patients aged > 75 years but effects on mental status were not reported [170,178,223]. A more recent RCT showed efficacy of fesoterodine in vulnerable elderly people with no differences in cognitive function at twelve weeks [224].
- Mirabegron: Analysis of pooled data from three RCTs showed efficacy and safety of mirabegron in elderly patients [225].
4.1.4.2.3.1. Applicability of evidence to the general elderly population
It is not clear how much the data from pooled and subgroup analyses from large RCTs can be extrapolated to a general ageing population. Community-based studies of the prevalence of anticholinergic adverse effects may be the most helpful [226]. When starting anticholinergics in elderly patients, mental function should be assessed and monitored [227]. No consensus exists as to the best mental function test to detect changes in cognition [207,228].
4.1.4.2.3.2. Anticholinergic burden
Several drugs have anticholinergic effects and, if another anticholinergic drug is prescribed, possible cumulative effects on cognition should be considered. Lists of drugs with anticholinergic properties are available from several sources [229].
Two SRs of largely retrospective cohort studies showed a consistent association between long-term anticholinergic use and cognitive dysfunction [230,231]. Longitudinal studies in older people over two to four years have found increased rates of cognitive decline in patients on anticholinergics or drugs with anticholinergic effects [199,200,232,233]. It is unclear whether there is a direct correlation between cognitive dysfunction caused by medication and the long-term risk of development of dementia.
4.1.4.2.3.3. Summary of evidence and additional recommendations for use of anticholinergic and beta-3 agonists in elderly patients
Summary of evidence | LE |
Anticholinergic drugs are effective in elderly women suffering from OAB/UUI. | 1b |
Mirabegron has been shown to be efficacious and safe in elderly women suffering from OAB. | 1b |
In older women the cognitive impact of drugs with anticholinergic effects is cumulative and increases with length of exposure. | 2 |
Oxybutynin may worsen cognitive function in elderly women. | 2 |
Darifenacin, fesoterodine, solifenacin and trospium have not been shown to cause cognitive dysfunction in elderly women in short-term studies. | 1b |
Recommendations | Strength rating |
Long-term anticholinergic treatment should be used with caution in elderly women, especially those who are at risk of, or have pre-existing cognitive dysfunction. | Strong |
Assess anticholinergic burden and associated co-morbidity in women being considered for anticholinergic therapy for overactive bladder syndrome. | Weak |
4.1.4.2.4. Oestrogens
Oestrogen treatment for UI has been tested using oral, transdermal, and vaginal routes of administration. Vaginal (local) treatment is primarily used to treat symptoms of vaginal atrophy in postmenopausal women. Available evidence is related mainly to SUI, and although some reviews include participants with UUI, it is difficult to generalise the results to women with predominantly OAB/UUI.
The association of LUTS with genitourinary syndrome of menopause (GSM) should be considered [234]. Genitourinary syndrome of menopause is a new term that describes various menopausal symptoms and signs associated with physical changes of the vulva, vagina and LUT. These include mucosal pallor/erythema, loss of vaginal rugae, tissue fragility/fissures, vaginal petechiae, urethral mucosal prolapse, introital retraction and vaginal dryness. There is evidence from a SR to suggest benefit from vaginal oestrogen therapy in GSM [235]. All vaginal oestrogens demonstrated superiority in objective and subjective end points of GSM compared with placebo. Only some trials demonstrated superiority vs. placebo in urogenital symptoms (UI, recurrent UTI, urgency, and frequency). No significant difference was observed between various doses and dosage forms of vaginal oestrogen products. Vaginal oestrogen showed superiority over vaginal lubricants and moisturisers for the improvement of objective clinical end points of vulvovaginal atrophy but not for subjective end points [235].
Available evidence suggests that vaginal treatment with oestradiol and oestriol is not associated with increased risk of thromboembolism, endometrial hypertrophy, and breast cancer that is seen with systemic
administration [236-238].
4.1.4.2.4.1. Summary of evidence and recommendation for oestrogen therapy
Summary of evidence | LE |
Vaginal oestrogen therapy may improve symptoms associated with GSM, of which OAB may be a component. | 1a |
Recommendation | Strength rating |
Offer vaginal oestrogen therapy to women with LUTS and associated symptoms of genitourinary syndrome of menopause. | Weak |
4.1.4.2.5. Placebo and nocebo
Placebo has a clear effect on the improvement of OAB signs and symptoms, and the overall placebo responses in various outcomes studied are statistically significant and, for some of the outcomes, possibly clinically significant. A recent SR including 57 studies with 12,901 patients showed a standardised mean difference of -0.45 for daily micturition episodes, -0.33 for daily nocturia episodes, -0.46 for UUI episodes, -0.50 for daily urgency episodes, -0.51 for daily incontinence episodes, and 0.25 for volume voided per micturition [239]. The same group published a SR with meta-analysis of data retrieved from 57 RCTs on the nocebo effect of pharmacotherapy in patients with OAB (up to 80% females). They reported dry mouth as the most common reported adverse event with mean rate of 4.9%, followed by constipation 2.6%. The authors concluded that HCPs should appreciate the possible positive and negative patient expectation regarding pharmacotherapy for OAB in order to optimise the individual outcomes [240]. The placebo response seems to be non-negligible in OAB, supporting the requirement for placebo control in RCTs.
4.1.4.3. Surgical management
4.1.4.3.1. Bladder wall injection of botulinum toxin A
OnabotulinumtoxinA (onabotA; BOTOX®) 100 U is licenced in Europe to treat OAB with persistent or refractory UUI in adults of both sexes [241,242]. Surgeons should be aware that other doses of onabotA and other formulations of botulinum toxin A, abobotulinumtoxin A and incobotulinumtoxin A, are not licensed for use in OAB/UUI. Doses for onabotA are not transposable to the other brands of onabotulinumtoxinA. The continued efficacy of repeat injections is usual, but discontinuation rates may be high [243,244]. The most important adverse events related to onabotA 100 U injection detected in the regulatory trials were UTI and an increase in PVR volume that may require CISC [245].
A SR included ten studies on 2,055 patients comparing intravesical onabotA injection with placebo. OnabotulinumtoxinA was more effective than placebo in improvement of mean symptoms score, reduction of mean urgency episodes, mean UUI episodes, mean frequency episodes, mean nocturia episodes [11]. No statistically significant difference was found between onabotA and placebo in change of mean voided volumes or maximum cystometric capacity.
OnabotulinumtoxinA was associated with significantly higher rates of voiding dysfunction compared to placebo at both 100 unit dose and 200 unit dose, and significantly higher rates of UTI both at 100-unit dose and 200-unit dose.
A Cochrane review reported no significant difference in PVR volume between the onabotA and placebo groups [246].
Quality of life was substantially improved in the onabotA arm, as shown by the > 2.5 times improvement in Incontinence Quality of Life Questionnaire (I-QOL) scores compared to baseline. Cohort studies have shown the effectiveness of bladder wall injections of onabotA in elderly and frail elderly people [247], although the success rate might be lower and the PVR volume (> 150 mL) higher in this group.
The median time to request retreatment in the pooled analysis of the two RCTs was 24 weeks [242,245]. Follow-up over 3.5 years showed consistent or increasing duration of effect for each subsequent treatment, with a median of 7.5 months. Considerable differences were noted in patients’ outcomes on secondary analysis [248].
Two RCTs on 545 patients compared onabotA injections with antimuscarinics. OnabotulinumtoxinA was significantly more effective in curing UUI, but no significant difference was noted in the reduction of mean UUI episodes. However, it was associated with significantly higher rates of voiding dysfunction than antimuscarinics, and UTIs [11].
Identification of DO in urodynamics does not appear to influence the outcome of onabotnA injections in patients with UUI [249].
4.1.4.3.1.1. Summary of evidence and recommendations for bladder wall injection of onabotulinumtoxinA
Summary of evidence | LE |
A single treatment session of onabotA (100 U) injected in the bladder wall is more effective than placebo at curing and improving UUI/OAB symptoms and improving QoL. | 1a |
There is no evidence that repeated injections of onabotA have reduced efficacy, but discontinuation rates are high. | 2a |
There is a risk of voiding dysfunction, increased PVR volume and UTI with onabotA injections. | 1a |
The risk of bacteriuria after onabotA (100 U) injection is high but the clinical significance of this remains uncertain. | 1b |
OnabotulinumtoxinA is more effective in curing UUI but similarly effective in reducing mean UUI episodes compared with antimuscarinics. | 1a |
OnabotulinumtoxinA is associated with higher rates of voiding dysfunction than antimuscarinics. | 1a |
Recommendations | Strength rating |
Offer bladder wall injections of onabotulinumtoxinA (100 U) to patients with OAB/UUI refractory to conservative therapy or drug treatment. | Strong |
Warn patients of the limited duration of response, risk of UTI and possible prolonged need for clean intermittent self-catheterisation prior to offering treatment with onabotulinumtoxinA. | Strong |
4.1.4.3.2. Sacral nerve stimulation
Sacral nerve stimulation (SNS) involves placing electrodes adjacent to the sacral nerve roots and delivering an electric current to the area via an attached battery implanted in the buttock. This delivers low-amplitude stimulation resulting in modulation of neural activity and stabilisation of bladder electrical activity through a mechanism that is, as yet, not fully understood. In most centres, test stimulation with a temporary or permanent electrode is performed to assess response, before undertaking permanent stimulator implantation. Currently, the only reliable predictor for treatment success in SNS is test stimulation. A SR did not find predictive factors of success due to low level of evidence of included studies (small, retrospective, and heterogeneous populations) [250].
All randomised studies suffer from the limitation that patients cannot be blinded to the treatment allocation since all recruited patients have to respond to a test phase before randomisation.
The ROSETTA trial randomised 386 women with refractory UUI to SNS (n = 194 women) or intradetrusor injection of onabotA (n = 192 women) [251]. At two years, the authors found no statistically significant difference between SNS and onabotA in improvement of mean symptom scores on OABq-SF or in reducing the mean UUI daily episodes. Patients reported significantly higher satisfaction with onabotA, but also significantly higher rates of recurrent UTIs than SNS (24% vs. 10%, respectively). On the other hand, SNS was associated with 9% removal rate and 3% revision rate at two-years follow-up.
The INSITE trial randomised 70 (94% women) patients to SNS implantation and 77 patients (92% women) to receive antimuscarinics [252]. At six months follow-up, results showed statistically significant higher success rate for SNS compared to antimuscarinics – success was defined as > 50% improvement in daily UUI or frequency episodes. Adverse events occurred in 30% and 27% of SNS and antimuscarinics trial arms, respectively, none were serious. SNS was associated with higher rates of UTIs and was associated with implant site infection and lead migration in 3.4% of cases each.
A Cochrane review [253] identified three RCTs that investigated SNS in patients with refractory UUI. The majority of studies compared a strategy of immediate implantation with delayed implantation. One study compared implantation to controls who stayed on medical treatment and received delayed implantation at six months. Fifty percent of the immediately implanted group had > 90% improvement in UUI at six months compared with 1.6% of the control group [254]. The effect on QoL measured by the SF-36, was unclear as it differed between the groups in only one of the eight dimensions. The other RCT achieved similar results, although these patients had already been included in the first report [255].
Another SR of studies including SNS with > 6 months follow-up reported dry rates of 43–56% [256]. Adverse events occurred in 50% of implanted cases, with surgical revision necessary in 33–41% [257,258]. In a sub-analysis of the RCT similar success rates were found in patients with or without urodynamic DO [259].
4.1.4.3.2.1. Summary of evidence and recommendation for sacral nerve stimulation
Summary of evidence | LE |
Sacral nerve stimulation is more effective than continuation of failed conservative treatment for OAB/UUI, but no sham controls have been used. | 1b |
Sacral nerve stimulation is as effective as onabotA 200 U injection at 24 months. | 1b |
In patients who have been implanted, 50% improvement of UUI is maintained in > 50% of patients and 15% may remain cured at four years. | 3 |
Recommendation | Strength rating |
Offer sacral nerve stimulation to patients who have overactive bladder/urge urinary incontinence refractory to anticholinergic therapy. | Strong |
4.1.4.3.3. Laser treatment
A recent SR evaluated the use of vaginal lasers in the treatment of OAB in short term studies detailing minimal improvement [260]. No RCTs were included, the quality of reported studies were weak and long-term safety data were also lacking.
4.1.4.3.3.1. Summary of evidence and recommendation for laser treatment
Summary of evidence | LE |
Vaginal laser therapy shows minimal OAB symptom improvement in the short term, with minimal complications, however, long-term efficacy and safety data is lacking. | 3 |
Recommendation | Strength rating |
Do not offer vaginal laser therapy to treat overactive bladder symptoms outside of a well-regulated clinical research trial. | Strong |
4.1.4.3.4. Cystoplasty/urinary diversion
4.1.4.3.4.1. Augmentation cystoplasty
In augmentation cystoplasty (also known as clam cystoplasty), a detubularised segment of bowel is inserted into the bivalved bladder wall. Most of the evidence pertaining to cystoplasty comes from patients with neuropathic bladder dysfunction. One study did not find any difference between bivalving the bladder in the sagittal or coronal plane [261,262]. The procedure can be done, with equal success by open or robotic techniques, although the latter takes more time [263].
There are no RCTs comparing bladder augmentation to other treatments for patients with OAB/UUI.
A large case series of bladder augmentation in a mixed population of idiopathic and neurogenic UUI included 51 women [264]. At an average follow-up of 74.5 months, only 53% were continent and satisfied with the surgery, whereas 25% had occasional leaks and 18% continued to have disabling UUI. The results for idiopathic DO (58%) were less satisfactory than for neurogenic UUI (90%). Malignant transformation was not reported in this series; however, it has been documented in other series and a SR [265-267]. Fewer than 60 cases have been reported worldwide, and almost all are exclusively beyond ten years after the original cystoplasty [268].
Adverse effects are common and have been summarised in a review with five to seventeen years follow-up
of > 267 cases; 61 of which had non-neurogenic UUI [269]. Short-term complications include bowel obstruction (2%), infection (1.5%), thromboembolism (1%), bleeding (0.75%) and fistula (0.4%). In the long term, patients may require CISC to obtain adequate bladder emptying (38%). Other long-term effects include asymptomatic bacteriuria (70%), changes in bowel symptoms (25%), UTI (20%), metabolic disturbances (16%), urinary tract stones (13%), deterioration in renal function (2%), and bladder perforation (0.75%).
It is unclear if mucolytic agents reduce mucus accumulation. The only RCT comparing various mucolytic agents did not find significant benefits with the use of N-acetylcysteine, aspirin, or ranitidine. In one small study (n = 40), subcutaneous octreotide immediately before, and for fifteen days after surgery yielded significant reductions in mucus production, the need for bladder irrigation to clear blockages, and mean duration of hospital stay [270]. Before cystoplasty, all potential complications should be outlined, and before and after surgery, patients should be well supported by stoma/continence nurses.
Depending on the relative costs of onabotA and augmentation cystoplasty, the latter can be cost-effective within 5 years if the complication rate is low and duration of effect of onabotA is < 5 months [271].
4.1.4.3.4.2. Detrusor myectomy (bladder auto-augmentation)
Detrusor myectomy aims to increase bladder capacity and reduce storage pressure by incising or excising a portion of the detrusor muscle, to create a bladder mucosal bulge or pseudo-diverticulum. It was initially described as an alternative to bladder augmentation in children [272].
Two case series in adult patients with idiopathic and neurogenic bladder dysfunction demonstrated poor long-term results caused by fibrosis of the pseudo-diverticulum [273,274]. This technique is rarely, if ever, used nowadays.
4.1.4.3.4.3. Urinary Diversion
Urinary diversion remains a reconstructive option for patients with intractable UI after multiple pelvic procedures, radiotherapy or pelvic pathology leading to irreversible sphincteric incompetence or fistula formation. Options include ileal conduit urinary diversion, orthotopic neobladder and heterotopic neobladder with Mitrofanoff continent catheterisable conduit. There is insufficient evidence to comment on which procedure leads to the most improved QoL.
A small study comparing ileal with colonic conduits concluded that there are no differences in the relative risks (RR) of UUT infection and uretero-intestinal stenosis. However, no studies have specifically examined these techniques for treatment of intractable OAB/UUI [261]. Therefore, careful consideration of which operation is undertaken depends on thorough preoperative counselling, access to stoma/continence nurses, as well as patient factors to allow for fully informed patient choice.
4.1.4.3.4.4. Summary of evidence and recommendations for cystoplasty/urinary diversion
Summary of evidence | LE |
There is limited evidence of the effectiveness of augmentation cystoplasty and urinary diversion specifically for treatment of idiopathic OAB or UUI. | 3 |
Augmentation cystoplasty and urinary diversion are associated with high risks of short- and long-term severe complications. | 3 |
The need to perform CISC following augmentation cystoplasty is common. | 3 |
There is no evidence comparing the efficacy or adverse effects of augmentation cystoplasty to urinary diversion. | 3 |
Recommendations | Strength rating |
Ensure patient counselling and life-long support both prior to and after major surgery as a treatment for overactive bladder (OAB) is provided by a specialist nurse or equivalent health care provider. | Strong |
Offer augmentation cystoplasty to patients with OAB/urge urinary incontinence (UUI) who have failed all other treatment options and have been informed about all possible complications. | Weak |
Inform patients undergoing augmentation cystoplasty of the high risk of clean intermittent self-catheterisation (ensure they are willing and able to do so) and that they will need life-long surveillance. | Strong |
Do not offer detrusor myectomy as a treatment for UUI. | Weak |
Only offer urinary diversion to patients who have failed less-invasive therapies for the treatment of OAB/UUI, who will accept a stoma and have been warned about the possible small risk of malignancy. | Weak |
4.1.5. Follow-up
Follow-up for women with OAB is guided by the type of treatment instituted and local service capacity. Standardisation of follow-up pathways can therefore be difficult. Here, we provide recommendations based on best practice and standards from clinical trials.
4.1.5.1. Recommendations for follow-up of patients with overactive bladder
Recommendations | Strength rating |
Offer early follow-up to women who have been commenced on anticholinergic or beta-3 agonist therapy. | Strong |
Offer repeat injections of onabotulinumtoxinA, as required, to women in whom it has been effective (refer to the manufacturer’s guidance regarding the minimum timeframe for repeat injections). | Strong |
Offer life-long surveillance to women who have a sacral nerve stimulation implant to monitor for lead displacement, malfunction, and battery wear. | Strong |
Offer cystoscopic surveillance to women with an augmentation cystoplasty due to the small risk of malignancy. | Weak |
4.2. Stress urinary incontinence
4.2.1. Epidemiology, aetiology, pathophysiology
Stress urinary incontinence, defined as the involuntary loss of urine on effort or physical exertion, is a significant health problem worldwide with social and economic impact on women and society. It is estimated that the number of women in the USA with UI will have increased from 18.3 million in 2010 to 28.4 million in 2050 [275]. The prevalence of SUI appears to peak between 45 and 59 years of age [276].
Data regarding the association of UI with ethnicity are conflicting. In several studies, SUI is more common in white women than in women of African American or Asian American origin [277,278]. Other factors positively associated with SUI include parity, obesity, previous hysterectomy or pelvic surgery, diabetes mellitus [279] and pulmonary disease [280]. Physical activity level is another important factor that is positively correlated with SUI severity [281]. A meta-analysis including six studies with a total sample size of 3,678 cases showed that the risk for SUI in women with metabolic syndrome was three times those without [282].
Two common, often overlapping, mechanisms for SUI have been described: (1) urethral hypermobility resulting from loss of support of the bladder neck and urethra; and (2) weakness of the urinary sphincter itself (intrinsic sphincter deficiency), which can result from trauma, radiotherapy, previous pelvic or uro-gynaecological surgery, neurological disease, or ageing.
The mechanism behind urethral hypermobility as a cause of SUI is based on the “vaginal hammock” hypothesis [283]. The endopelvic fascia, which is attached to the upper (abdominal) side of the PFMs, links the muscles to the vagina and represents the “hammock”, which can compress the urethra during rest and activity. This compression, combined with intrinsic urethral sphincter pressure, supports, and maintains the urethra in the correct and closed position, preventing involuntary loss of urine, despite any increases in intravesical pressure. Damage to the supporting tissues (particularly the arcus tendinous fasciae pelvis, the central part of the fascia) can result in urethral hypermobility. Consequently, rather than being compressed at times of increased intra-abdominal pressure, the urethra moves caudally, funnelling the bladder neck, and is no longer compressed, resulting in SUI [283,284]. In general, almost all treatments are used for both subtypes of SUI, but in general most treatments are more successful in patients with some degree of urethral hypermobility than for isolated intrinsic weakness of the urinary sphincter [285].
4.2.2. Classification
Patients with SUI can be classified as uncomplicated and complicated [286]. The Panel has reached a consensus on the definition to be used throughout this guideline document:
- Women with uncomplicated SUI: no prior surgery for SUI, extensive pelvic surgery, or pelvic radiotherapy; no neurogenic LUT dysfunction; no bothersome genitourinary prolapse; absence of voiding symptoms; and no medical conditions that affect the LUT. In cases where additional significant storage symptoms, especially OAB, are present, consider a possible diagnosis of MUI (see Section 4.3).
- Women with complicated SUI: previous surgery for incontinence or extensive pelvic surgery; history of pelvic irradiation; presence of anterior or apical POP; presence of voiding symptoms or neurogenic LUT dysfunction; significant OAB/UUI; congenital abnormalities such as bladder exstrophy. Neurogenic LUT dysfunction is reviewed in the EAU Guidelines on Neuro-Urology and will not be considered further in these guidelines [9]. The treatment of LUTS associated with genitourinary prolapse has been included in these guidelines (see Section 4.7).
4.2.3. Diagnostic evaluation
4.2.3.1. History and physical examination
There is universal agreement that taking a history, should be the first step in the assessment of anyone with UI. When the history categorises UI as probable SUI the presence of complicated or uncomplicated SUI can also be determined. Those patients who require rapid referral to an appropriate specialist can also often be identified from the clinical history.
There is little evidence from clinical trials that carrying out a clinical examination improves clinical outcomes, but there is widespread consensus that it remains an essential part of the assessment of women with SUI. It should include abdominal examination, vaginal examination and careful assessment of any associated POP, examination of the perineum and evaluation of PFM strength, as well as a neuro-urological examination. An attempt to reproduce the SUI should be made. A standing cough test has greater sensitivity for diagnosis of SUI compared with a supine cough test [287]. Despite this, the ICS has proposed a standardisation of the female cough stress test that includes a supine/lithotomy position with 200–400 mL fluid in the bladder and one to four coughs [288].
4.2.3.1.1. Summary of evidence and recommendation for history and physical examination
Summary of evidence | LE |
A standing cough stress test is more sensitive than a supine test. | 1b |
Recommendation | Strength rating |
Take a full clinical history and perform a thorough physical examination including standardised cough stress test in all women presenting with stress urinary incontinence. | Strong |
4.2.3.2. Patient questionnaires
Although many studies have investigated the validity and reliability of urinary symptom questionnaires and PROMs, most of these studies did not include homogeneous populations of adult women diagnosed with SUI. This limits the extent to which results and conclusions from these studies can be specifically applied to women with SUI. Some questionnaires are used for prevalence studies; others are responsive to change and may be used to measure outcomes, although evidence on their sensitivity is inconsistent [26,27]. There is no evidence to indicate whether use of QoL or condition-specific questionnaires has an impact on treatment outcome. To date, there is not one questionnaire that fulfils all requirements for the assessment of women with SUI.
4.2.3.2.1. Summary of evidence and recommendation for patient questionnaires
Summary of evidence | LE |
Validated condition-specific symptom scores assist in the screening for and categorisation of UI. | 3 |
Validated symptom scores measure the severity and associated bother of SUI. | 3 |
Both condition-specific and general health status questionnaires measure current health status and are responsive to change following treatment. | 3 |
Recommendation | Strength rating |
Use a validated and appropriate questionnaire as part of the standardised assessment of patients with stress urinary incontinence. | Strong |
4.2.3.3. Post-void residual volume
It is important to evaluate PVR volume in patients with SUI; particularly in those who also have voiding symptoms or POP. The prevalence of a significant PVR volume in patients with SUI is uncertain, partly because of the lack of a standard definition of an abnormal PVR volume. Most studies investigating PVR volume have not included patients with SUI. In general, the data on PVR volume can only be applied with caution to adults with non-neurogenic SUI. In a cohort study of > 900 women with SUI, there was good correlation between PVR volume estimated by US and measured by catheterisation [59].
4.2.3.3.1. Summary of evidence and recommendations for post-void residual volume
Summary of evidence | LE |
The majority of women with SUI do not have a significant PVR volume. | 3 |
There is good correlation between PVR volume estimated using US and measured via catheterisation in women with SUI. | 3 |
Recommendations | Strength rating |
Measure post-void residual (PVR) volume, particularly when assessing patients with voiding symptoms or complicated stress urinary incontinence (SUI). | Strong |
When measuring PVR volume, use ultrasound in preference to catheterisation. | Strong |
Monitor PVR volume in patients scheduled for treatment that may cause or worsen voiding dysfunction, including surgery for SUI. | Strong |
4.2.3.4. Urodynamics
The role of urodynamics in SUI evaluation remains poorly defined and is still under debate.
Invasive urodynamic tests are often performed prior to surgical treatment of SUI. Clinical diagnosis of incontinence and cystometric findings often do not correlate [66,67]. The diagnostic accuracy of urethral pressure profilometry [68] and VLPP measurement in SUI is generally poor [289]. Measurement of MUCP correlates, albeit weakly, with incontinence severity [68], and there is conflicting evidence about its reproducibility [64,65]. Methods of recording MUCP cannot be compared meaningfully [290]. Valsalva leak point pressures are not standardised and there is minimal evidence about reproducibility. Valsalva leak point pressures did not reliably assess incontinence severity in a cohort of women selected for surgical treatment of SUI [69]. The predictive value of the tests regarding treatment outcome remains unclear.
A Cochrane review including seven RCTs showed that urodynamic tests increased the likelihood of avoiding surgery for SUI. However, there is no evidence that this influence on decision-making alters the clinical outcome of treatment within trial populations [77].
A high-quality RCT (n = 630) compared office evaluation alone and combined with urodynamics in women with clinically demonstrable SUI about to undergo surgery. While urodynamics changed the clinical diagnosis in 56% of women [291], there was no difference in severity of SUI or any secondary outcome at twelve months’ follow-up after SUI surgery [79]. A similar study also found that omission of urodynamics in the preoperative work-up of SUI did not lead to inferior results [292]. Patients in whom urodynamics were discordant with clinical assessment (n = 109) were randomly allocated to receive either immediate surgery or individually tailored therapy based on the urodynamic findings. In this trial, performing immediate surgery, irrespective of the result of urodynamics, did not result in inferior outcomes [293]. An RCT, in which 145 women were randomised to retropubic or trans-obturator MUS, concluded that when patients were stratified according to preoperative VLPP (< or > 60 cm H2O), it was not linked to outcome after both synthetic MUS procedures [294].
Another study reported conflicting evidence. Valsalva leak point pressures or MUCP in the lowest quartile was predictive in terms of synthetic MUS failure at twelve months [83].
The Panel recognises that it may be valuable to use urodynamic test results to help select the optimum surgical procedure, but the evidence outlined above suggests that performing urodynamics in patients with uncomplicated SUI, which can be diagnosed based on detailed clinical history and demonstrated at examination, is not necessary. The role of urodynamics in complicated SUI is still under debate [295]. However, the Panel consensus is that urodynamics should be carefully considered in cases of SUI with associated storage symptoms; cases in which the type of incontinence is unclear; cases in which voiding dysfunction is suspected; and cases with associated POP or prior surgery for SUI. This is in line with other guideline documents in this area [66].
4.2.3.4.1. Summary of evidence and recommendations for urodynamics
Summary of evidence | LE |
Preoperative urodynamic testing in women with uncomplicated, clinically demonstrable, SUI does not improve surgical outcome for SUI. | 1b |
There is no consistent correlation between urethral function tests and subsequent success or failure of SUI surgery. | 3 |
There is no consistent evidence that preoperative DO is associated with surgical failure of MUS in women. | 3 |
Recommendations | Strength rating |
Perform preoperative urodynamic tests in cases of SUI with associated storage symptoms, cases in which the type of incontinence is unclear, cases in which voiding dysfunction is suspected, and cases with associated pelvic organ prolapse or prior surgery for SUI. | Weak |
Perform urodynamic tests if the findings may change the choice of invasive treatment. | Weak |
Do not use urethral pressure profilometry or leak point pressure to grade severity of incontinence as they are primarily tests of urethral function. | Strong |
4.2.3.5. Pad testing
Please refer to Section 3.7 for the diagnostic accuracy and predictive value of using pad testing to quantify the presence and severity of SUI. The summary of evidence and recommendations can be found in section 3.7.1.
4.2.3.6. Imaging
The role of imaging in SUI patients is limited. Many studies have evaluated imaging of bladder neck mobility by US and MRI and concluded that SUI cannot be identified by a particular pattern of urethro-vesical movement [296].
In addition, the generalised increase in urethral mobility after childbirth does not appear to be associated with de novo SUI [297]. Studies have assessed the use of imaging to investigate the mechanism of action of MUS inserted for SUI. One study suggested that MUS placement decreased mobility of the mid-urethra but not mobility of the bladder neck [109]. Following MUS surgery, a wider gap between symphysis and sling (assessed by imaging) has been shown to correlate with a lower chance of cure of SUI [110]. One study of 72 women post-synthetic sub-urethral MUS surgery has investigated the usefulness of trans-labial US to assess tape functionality. In this study different parameters were measured (distance from tape to urethra, position, and shape during Valsalva manoeuvre, etc.) and concluded that tape position relative to the patient’s urethra seems to play a role in treatment outcome [298]. The general role of US in the evaluation and follow-up of women with SUI is unclear, and further research is needed to establish its place in the clinical pathway.
Several imaging studies have investigated the relationship between sphincter volume and function [299] and sphincter volume and outcome of surgery [300] in women. However, no imaging test has been shown to predict the outcome of treatment for SUI. Imaging of the pelvic floor can identify levator ani detachment and hiatus size, although there is little evidence of a relationship to clinical benefit after treatment of SUI.
4.2.3.6.1. Summary of evidence and recommendation for imaging
Summary of evidence | LE |
Imaging can reliably be used to measure bladder neck and urethral mobility, although there is no evidence of clinical benefit for patients with UI. | 2b |
Recommendation | Strength rating |
Do not carry out imaging of the upper or lower urinary tract as part of the routine assessment of stress urinary incontinence. | Strong |
4.2.4. Disease management
4.2.4.1. Conservative management
4.2.4.1.1. Obesity and weight loss
Being overweight or obese has been identified as one of the risk factors for LUTS and SUI in many epidemiological studies [136,137]. There is evidence that the prevalence of both UUI and SUI increases proportionately with BMI [301]. The proportion of patients who undergo surgery for incontinence who are overweight or obese is higher than that of the general population [137]. On the other hand, young, elite athletes, and women who work-out for fitness show a high prevalence of UI/SUI [281,302].
Three SRs concluded that weight loss was beneficial in improving UI [135,136,303]. Five further RCTs reported a similar beneficial effect on incontinence following surgical weight reduction programmes [304-308].
In a prospective study in 160 consecutive women who underwent bariatric surgery, surgically induced weight loss was associated with a significant improvement in pelvic floor disorders, including UI [309]. Similar results reported by prospective single-centre studies investigating the effect of weight loss induced by bariatric surgery revealed that bariatric surgery was associated with substantially reduced UI at eleven months and three years [310,311].
4.2.4.1.1.1. Summary of evidence and recommendation for obesity and weight loss
Summary of evidence | LE |
Obesity is one of the risk factors for LUTS and UI in women. | 3 |
Non-surgical weight loss improves UI in overweight and obese women. | 1a |
Surgical weight loss improves UI in obese women. | 1b |
Recommendation | Strength rating |
Encourage overweight and obese women with LUTS/stress urinary incontinence to lose weight and maintain weight loss. | Strong |
4.2.4.1.2. Urinary containment
The evidence for urinary containment derives from the same literature as for containment in OAB-wet. The readers are therefore referred to Section 4.1.4.1.3. The summary of evidence and recommendations for urinary containment can be found in Section 4.1.4.1.3.1.
4.2.4.1.3. Pelvic floor muscle training
Pelvic floor muscle training is used to improve functional and morphological parameters of the pelvic floor, thus improving urethral stability.
An immediate effect of a single PFM contraction is narrowing of the levator hiatus area, increase of urethral closure pressure, and lifting of the bladder and rectum thus preventing occurrence of SUI [312-314]. In an RCT comparing intensive PFMT over a six-month period with no treatment, there were increased muscle strength and endurance, narrowing of the levator hiatus, reduced PFM length, increased muscle volume, and lifting of the bladder neck and rectal ampulla [315]. Pelvic floor muscle training may be used to prevent SUI, e.g., in childbearing women before birth, or as part of a planned recovery programme after childbirth. Most often, PFMT is used to treat existing SUI; sometimes in combination with observation and/or palpation of the muscle contraction by the therapist, or biofeedback (using an apparatus measuring the contraction either by electromyography, manometry, dynamometry, US or MRI). Electrical stimulation and vaginal cones are also used in treatment of SUI based on an assumption of the same mechanism of action.
4.2.4.1.3.1. Efficacy of pelvic floor muscle training
A Cochrane review compared PFMT with no treatment or inactive control treatment and found that women with SUI in the PFMT groups were eight times more likely to report cure [316]. The review also documented significant improvement in SUI and improvement in UI QoL. Pelvic floor muscle training reduced leakage by an average of one episode per day in women with SUI. Women with SUI in the PFMT groups lost significantly less urine in short (up to one-hour) pad tests. The comparison of short pad tests showed considerable heterogeneity, but the findings still favoured PFMT when using a random-effects model. Women in the PFMT group were also more satisfied with treatment and their sexual outcomes were better. Adverse events were rare and minor.
A Cochrane review concluded that there may be some additional effect of adding biofeedback to PFMT. However, this was based on RCTs with training frequency and attention favouring biofeedback [317]. In a recent RCT (61.3% had MUI) comparing the exact same training dosage and attention between groups, use of biofeedback did not yield any additional effect [318]. Group training is cost-effective in treatment of SUI/UI compared to individual treatment [319]. Another Cochrane review concluded that combination of individual assessment/education and group training was equally effective compared to individual treatment, but again the dosage and attention differed between comparison groups [320]. In a more recent RCT with the exact same training dosage and attention in individual and group training, group training was not inferior to individual treatment [319]. It is worth noting that all of the PFMT interventions in these reviews follow individual assessment and teaching before starting PFMT, and most interventions use some sort of measurement tool (biofeedback) in the assessment.
Both the Cochrane review and the ICI concluded that the use of vaginal cones to train the PFMs is more effective than no treatment, but it is inconclusive whether it is more or less effective than structured
PFMT [316,321,322]. Some women are unable to maintain the cone inside, and some report discomfort and motivation problems and adherence may be low [321].
The Cochrane review [316], the ICI [322] and the National Institute for Health and Care Excellence (NICE) guidelines (2019) [66] all conclude that there is the highest level evidence (1a) to support PFMT in the treatment of SUI/MUI. All SRs conclude that PFMT is less effective if women with MUI and UUI are included in the studies and more effective with more intensive and supervised training. According to the NICE guidelines literature review, PFMT is as effective as surgery for around half of women with SUI, and due to the risks following surgery and absence of adverse effects of PFMT, they recommend three months of supervised PFMT as first-line treatment for SUI and MUI [66].
Pelvic floor muscle training was compared to synthetic MUS surgery in an RCT involving 460 women with moderate to severe SUI [323]. Crossover between treatment arms was allowed and 49% of women in the physiotherapy group and 11.2% of women in the surgery group crossed over to the alternative treatment. Subjective improvement was reported by 90.8% of women in the surgery group and 64.4% of women in the physiotherapy group at twelve months [323].
4.2.4.1.3.2. Efficacy of electrical stimulation
There is lack of consensus regarding the use of ES to treat SUI. For subjective cure of SUI, a Cochrane review found moderate-quality evidence that ES is probably better than no active treatment [324]. Similar results were found for cure or improvement of SUI, but the quality of evidence was low. There is uncertainty as to whether there is a difference between ES and sham treatment in terms of subjective cure alone because of the very low quality of evidence. For subjective cure or improvement, ES may be better than sham treatment. Any comparison between ES and PFMT and other treatments is hampered by low-quality evidence. One assessor blinded RCT found that PFMT was significantly better than either the use of vaginal cones or electrical stimulation. Only PFMT showed improvement in PFM strength and SUI measured by pad test and leakage episodes compared to control [325]. Adverse effects such as pain and discomfort have been reported, and ES is not tolerated by all women [324].
In an RCT, 132 women assessed by vaginal palpation to have 0–1 on the modified Oxford grading scale (unable to contract the PFM) were randomly assigned to an eight-week intervention of learning to contract via palpation, palpation with pelvic tilt, intravaginal ES, or verbal instruction [326]. The results showed that 63.6%, 69.7%, 33.3% and 18.2% in the four groups, respectively, scored 2 after the intervention. Palpation was significantly more effective that ES, but one third of the ES group had learned a correct PFM contraction [326]. The effect on UI measured by ICIQ-UI-SF was significantly better in the palpation group. An RCT [327] compared electrical stimulation with untreated control in 64 women with 0-1 on the modified Oxford grading scale. After the intervention, the ability to contract the PFMs was acquired by 36% of the experimental group and 12% of the control group. The experimental group also improved by a mean of 2 points more than the control group on the ICIQ-UI-SF score.
4.2.4.1.3.3. Long-term efficacy of pelvic floor muscle training
In a SR including nineteen studies, 1,141 women were followed-up for one to fifteen years after PFMT for SUI [328]. Meta-analysis was not performed due to high heterogeneity of outcome measures and training dosage (frequency, intensity, duration, and adherence). Only two studies provided interventions during follow-up. Losses to follow-up ranged between 0% and 39%. Long-term adherence to PFMT varied between 10% and 70%. Five studies reported that the initial success rate on SUI and MUI was maintained in the long term. Long-term success based on responders in the original trial varied between 41% and 85%. Surgery rates in the long term varied between 4.9% and 58%. It was concluded that short-term outcome of PFMT can be maintained at long-term follow-up without incentives for continued training, but there is a high heterogeneity in both interventional and methodological quality in short- and long-term PFMT studies [328].
4.2.4.1.3.4. Efficacy of pelvic floor muscle training in childbearing women
Pelvic floor muscle training to prevent SUI has been studied during pregnancy and in the postpartum period and the results are not reported separately for SUI and other subgroups of UI. A Cochrane review concluded that PFMT in women with and without UI (combined primary and secondary prevention) during pregnancy, produced a 26% reduced risk of UI during pregnancy and the mid-postnatal period [329]. Furthermore, pregnant continent women (primary prevention) who exercised the PFM during pregnancy were 62% less likely to experience UI in late pregnancy and had 29% lower risk of UI three to six months after giving birth. There is insufficient evidence for a long-term effect of antenatal PFMT beyond six to twelve months postpartum. Compared with usual care, there is no evidence that antenatal PFMT in incontinent women decreases incontinence in late pregnancy (very low-quality evidence), or in the mid- (low-quality evidence) or late postnatal periods (very low-quality evidence).
There have been fewer RCTs in the postpartum period than during pregnancy [329]. No primary prevention studies were found in women after birth. For PFMT started after delivery, in a mixed group of continent and incontinent women, there was uncertainty about the effect on UI risk in the late postnatal period (three trials, 826 women; moderate-quality evidence), and in postnatal women with persistent UI, there is no evidence that PFMT results in a difference in UI at more than six to twelve months postpartum (three trials; 696 women; low-quality evidence). However, another RCT found that UI was less frequent in the intervention group, with 57% of patients still symptomatic, compared to 82% of controls, as was bladder-related problems with a prevalence of 27% in the intervention vs. 60% in the control group [330]. Randomised controlled trials of high interventional and methodological quality are needed in the postpartum period.
4.2.4.1.3.5. Efficacy of Pelvic floor muscle training in elderly women
There have been few RCTs on conservative treatment of SUI in elderly women (> 65 years) and many of the studies combined different modalities, such as BT, lifestyle modifications and PFMT [331]. Some of the studies on PFMT and SUI in the general population have included women > 65 years and PFMT seems to be equally effective in elderly women. A SR on conservative management included 23 trials, with nine of moderate-to-high methodological quality and concluded that PFMT in combination with physical training was effective in reducing UI and improving QoL [332]. Prompted voiding and toileting assistance with functional exercise reduced UI. Other behavioural interventions such as night-time prompted voiding and waking routine had no effect on UI reduction. The most recent ICI consensus publication stated that although there are limited studies of PFMT on UI in frail elderly populations, age and frailty alone should not preclude the use of PFMT in appropriate patients with sufficient cognition to participate [331]. More high-quality RCTs, both in frail and healthy older women (> 80 years of age) are needed.
4.2.4.1.3.6. Composite treatments for PFMT
A Cochrane review found insufficient evidence to state whether there were additional effects by adding PFMT to other active treatments (including vaginal cones, electromagnetic stimulation, biofeedback, continence pessary, drugs) when compared with the same active treatment alone for female SUI or mixed UI. However, these results should be interpreted with caution as most of the comparisons were investigated in small, single trials. Also, none of the included trials reported data on adverse events associated with the PFMT regimen, thereby making it very difficult to evaluate the safety of PFMT [333].
A single-blind RCT evaluated whether peri-operative supervised PFMT was superior to standard care (handout) in terms of improvements in SUI symptoms, cure rate, and/or post-operative filling or voiding symptoms among women undergoing synthetic MUS insertion for SUI. The results showed that supervised PFMT improves SUI cure rates associated with synthetic MUS insertion with OR > 3 when considering symptoms of SUI, but does not improve post-operative continence function as measured by a pad test, nor does it lead to fewer post-operative voiding or filling symptoms [334].
4.2.4.1.3.7. Summary of evidence and recommendations for pelvic floor muscle training
Summary of evidence | LE |
Pelvic floor muscle training is better than no treatment for improving SUI and QoL in women with SUI and MUI across a range of outcomes, including cure rate, improvement rate, QoL, number and volume of urine leaks and treatment satisfaction. | 1a |
Pelvic floor muscle training exhibits a low rate of adverse events. | 1a |
Higher-intensity, supervised treatment regimens confer greater benefit in women receiving PFMT. | 1a |
There is no extra benefit of combining PFMT with biofeedback. | 1b |
Short-term benefits of intensive PFMT can be maintained in the long term. | 2a |
Pelvic floor muscle training in the antenatal period is associated with a reduced risk of UI in late pregnancy and in the short term postnatally. | 1a |
Postpartum PFMT is effective in women with persistent UI. | 1b |
The benefit of postpartum PFMT in mixed populations (continent and incontinent) of women is uncertain. | 1b |
Mid-urethral sling surgery is superior to PFMT in women with moderate-to-severe SUI. | 1b |
Pelvic floor muscle training commencing in the early postpartum period improves UI in women for up to six months. | 1b |
There is conflicting evidence on whether the addition of ES increases the effectiveness of PFMT alone. | 2a |
There is low to moderate certainty evidence suggesting benefit of ES in patients with SUI. In addition, ES may be useful for learning a correct PFM contraction. | 1b |
Recommendations | Strength rating |
Offer supervised intensive pelvic floor muscle training (PFMT), lasting at least three months, as first-line therapy to all women with stress urinary incontinence (SUI) or mixed urinary incontinence (including elderly women and pre- and postnatal women). | Strong |
Ensure that PFMT programmes are as intensive as possible. | Strong |
Balance the efficacy and lack of adverse events from PFMT against the expected effect and complications from invasive surgery for SUI. | Strong |
Consider electrical stimulation for treatment of SUI, or as an adjunct for teaching PFM contraction. | Weak |
4.2.4.1.4. Electromagnetic stimulation
Electromagnetic stimulation (EMS) has been evaluated for its role in SUI therapy. In a double-blind RCT of EMS including 70 women with SUI, no effect of EMS over sham in any outcome was recorded [335].
4.2.4.1.5. Electroacupuncture
A SR including 15 RCTs and women with SUI treated by electroacupuncture (EA) demonstrated that EA for SUI was effective. The ICIQ-SF scores improved, and 1-hour urine leakage decreased in patients undergoing EA compared with those receiving sham EA, physical exercise or medication [336].
4.2.4.2. Pharmacological management
4.2.4.2.1. Oestrogen
Oestrogenic drugs including conjugated equine oestrogens, oestradiol, tibolone and raloxifene, are used as hormone replacement therapy (HRT) for women with natural or therapeutic menopause.
Oestrogen treatment for SUI have been tested using oral, transdermal, and vaginal routes of administration. Available evidence suggests that vaginal oestrogen treatment with oestradiol and oestriol is not associated with the increased risk of thromboembolism, endometrial hypertrophy, and breast cancer seen with systemic administration [236-238]. Vaginal (local) treatment is primarily used to treat symptoms of vaginal atrophy in postmenopausal women.
A Cochrane SR looked at the use of oestrogen therapy in postmenopausal women given local oestrogen therapy and seventeen studies focused on SUI [236]. There is also a narrative review of oestrogen therapy in urogenital diseases [337]. The Cochrane review found that vaginal oestrogen treatment improved symptoms of SUI in the short term [236]. There were small, low-quality trials comparing vaginal oestrogen treatment with phenylpropanolamine, PFMT, ES and its use as an adjunct to surgery for SUI. Local oestrogen was less likely to improve UI than PFMT but no differences in UI outcomes were observed for the other comparisons. A single trial of local oestrogen therapy comparing a ring device to pessaries found no difference in UI outcomes, although more women preferred the ring device. In one trial, no significant adverse effects following vaginal administration of oestradiol for vulvovaginal atrophy over a two year period were reported [338].
Vaginal oestrogen therapy can be given as conjugated equine oestrogen, oestriol or oestradiol in vaginal pessaries, vaginal rings, or creams. The ideal treatment duration and the long-term effects are uncertain. A review of local oestrogen treatment showed improvement of UI over placebo with vaginal rings, which were favoured subjectively over pessaries [339].
One RCT in postmenopausal women showed a benefit of adding intravaginal oestriol to vaginal ES and PFMT in female SUI [340].
Studies of systemic HRT with non-urogenital primary outcomes have looked for change in urinary continence in secondary analyses. Large trials using conjugated equine oestrogens showed a higher rate of development or worsening of UI compared to placebo and no SUI improvement [341-346]. In a single RCT, use of raloxifene was not associated with development or worsening of UI [347]. Two small RCTs using oral oestriol or oestradiol as HRT for vulvovaginal atrophy suggested that UI symptoms were improved although the evidence was unclear [66,348].
4.2.4.2.1.1. Summary of evidence and recommendations for oestrogens
Summary of evidence | LE |
Vaginal oestrogen therapy improves SUI for postmenopausal women in the short term. | 1a |
Neoadjuvant or adjuvant use of local oestrogens is ineffective as an adjunct to surgery for SUI. | 2b |
Systemic HRT using conjugated equine oestrogens does not improve SUI and may worsen | 1a |
Recommendations | Strength rating |
Offer vaginal oestrogen therapy to postmenopausal women with stress urinary incontinence (SUI) and symptoms of vulvovaginal atrophy. | Strong |
In women taking oral conjugated equine oestrogen as hormone replacement therapy (HRT) who develop or experience worsening SUI, discuss alternative HRT. | Strong |
4.2.4.2.2. Duloxetine
Duloxetine inhibits the presynaptic reuptake of neurotransmitters, serotonin (5-hydroxytryptamine; 5-HT) and noradrenaline (NE).
In the sacral spinal cord, an increased concentration of 5-HT and NE in the synaptic cleft increases stimulation of 5-HT and NE receptors on the pudendal motor neurons, which in turn increases the resting tone and contraction strength of the urethral striated sphincter.
Duloxetine was evaluated as a treatment for female SUI or MUI in three SRs [171,349,350]. Improvement in UI compared to placebo was observed with no clear differences between SUI and MUI. One study reported cure for UI in 10% of patients. An improvement in the UI QoL questionnaire was not found in the study, which used this as a primary endpoint. In a further study comparing duloxetine, 80 mg daily, with PFMT alone,
PFMT + duloxetine, and placebo [351], duloxetine reduced leakage compared to PFMT or no treatment. Global improvement and QoL were better for combined therapy than no treatment. There was no significant difference between PFMT and no treatment in this trial.
Two open-label studies with a follow-up of > 1 year evaluated the long-term effect of duloxetine in controlling SUI [352,353]. Both studies had a high patient withdrawal rate, due to lack of efficacy and a high incidence of adverse events, including nausea and vomiting (> 40% of patients), dry mouth, constipation, dizziness, insomnia, somnolence, and fatigue.
A SR showed significant efficacy for duloxetine compared to placebo in women with SUI, but with increased risk of adverse events [350]. The adverse effects of duloxetine include mental health problems and suicidal ideation. A meta-analysis of four RCTs including 1,910 women with SUI reported no suicidality, violence, or akathisia events, but suggested that discontinuation rate due to adverse events was around one in seven and that the harm may outweigh the benefit of treatment [354]. A meta-analysis of twelve placebo-controlled trials involving almost 3,000 patients showed that in patients with major depressive disorders there were no significant differences in the incidence of suicide-related events with duloxetine vs. placebo [355].
4.2.4.2.2.1. Summary of evidence and recommendations for duloxetine
Summary of evidence | LE |
Duloxetine improves SUI in women, but the chances of cure are low. | 1a |
Duloxetine may cause significant gastrointestinal and central nervous system adverse effects, leading to a high rate of treatment discontinuation, although these symptoms may be limited to the first weeks of treatment. | 1a |
Recommendations | Strength rating |
Offer duloxetine (where licensed) to selected patients with stress urinary incontinence unresponsive to other conservative treatments and who want to avoid invasive treatment, counselling carefully about the risk of adverse events. | Strong |
Duloxetine should be initiated and withdrawn using dose titration because of the high risk of adverse events. | Strong |
4.2.4.2.3. Adrenergic agonists
A Cochrane SR including 22 RCTs involving 673 women and seven different adrenergic drugs (phenylpropanolamine in eleven trials, midodrine in two, norepinephrine in three, clenbuterol in another three, terbutaline in one, eskornade in one and Ro 115-1240 in one) found weak evidence that adrenergic agonists may improve SUI. Moreover, side effects did occur but were usually minor. More evidence is needed to compare adrenergic drugs with other drugs for SUI and, also with PFMT [356].
4.2.4.3. Surgical management
4.2.4.3.1. General considerations
The use of polypropylene mesh as synthetic MUS for the treatment of SUI has recently come under scrutiny following concerns about long-term complications. In some European countries such as the UK, the use of synthetic MUS has been paused and pelvic mesh was the subject of a parliamentary review published in July 2020 [357]. This review concluded that “For many women mesh surgery is trouble free and leads to improvements in their condition. However, this is not the case for all. There is no reliable information on the true number of women who have suffered complications. While they may be in the minority, that does not diminish the catastrophic nature of their suffering or the importance of providing support to them and learning from what has happened to them”.
The range of complications highlighted during the process of this parliamentary review included [357]:
- pain;
- recurrent infections;
- mobility issues;
- recurring or new incontinence/urinary frequency;
- recurring or new prolapse;
- haemorrhage;
- bowel issues;
- erosion of mesh; this can be into the vagina and/or other organs;
- sexual difficulties; including pain on intercourse and a loss of sex life;
- autoimmune issues;
- psychological impacts.
When considering the choice of surgical treatments for SUI the Panel advises individual clinicians to abide by any national or local rules that may be in place regarding mesh surgery. It is essential for clinicians to point out the deficiencies in the long-term evidence regarding mesh use in SUI with specific reference to the complications highlighted above.
In line with the recommendations from NICE [66] and the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) paper [358], the Panel agrees that surgeons and centres performing surgery should:
- be trained in the field of incontinence and for each surgical procedure they perform/offer;
- perform sufficient numbers of a procedure to maintain expertise of him/herself and the surgical team;
- be able to offer alternative surgical treatments;
- be able to deal with the complications of surgery;
- provide suitable arrangements for long-term follow-up.
The establishment of accurate and complete databases registering the interventions, patient profiles and surgical complications or all surgical treatments for SUI is recommended to allow the generation of robust long-term data.
Many surgical procedures are available for uncomplicated SUI patients and the Panel analysed the results of the different procedures in terms of clinical effectiveness, safety and cost-effectiveness based on the recent ESTER SR and economic evaluation [359] and previous SRs including those from the Cochrane Collaboration [360-364].
The outcome parameters used to evaluate surgery for SUI have been limited to:
- continence rate;
- patient-reported outcome measures;
- general and procedure-specific complications;
- generic, specific (UI) and associated (sexual and bowel) QoL.
In this context, it has to be taken into account that a number of products may no longer be available and therefore the recommendations may not be transferable to current devices. The Panel makes a strong recommendation that new devices are only used as part of a structured research programme and their outcomes monitored in a registry, until there is adequate evidence of safety and efficacy.
4.2.4.3.1.1. Shared decision making
The Panel recognises that a shared decision-making approach is paramount when any treatments are proposed but felt particular emphasis should be made for the topic area of surgical treatment for SUI. There are a number of different options available for patients which vary in both efficacy and safety profile. Consequently, the amount of information given to patients considering surgery for SUI is substantial. The Panel would unequivocally advise adherence to the fundamental principles of the shared decision-making process which include:
- full participation from the patient;
- delivery of factual information regarding benefits and risks of any particular treatment, if possible adapted to the specific situation of the patient;
- delivery of information about the experience and expertise of the HCP/institution delivering the treatment, especially for highly specialised procedures such as complex SUI and mesh removal surgery;
- confirmation that the patient understands the information given;
- clinician understanding and documenting individual patient preferences;
- facilitation of deliberation and initial decision-making;
- patient opportunity to consider and confirm any decisions made;
- clinician assistance with implementation of the final decision.
4.2.4.3.1.2. Recommendations for surgical treatment
Recommendations | Strength rating |
Offer patients who have explored/failed conservative treatment options a choice of different surgical procedures, where appropriate, and discuss the advantages and disadvantages of each approach. | Strong |
Use new devices for the treatment of stress urinary incontinence (SUI) only as part of a structured research programme. Their outcomes must be monitored in a registry or as part of a well-regulated research trial. | Strong |
Employ a shared decision-making approach when deciding on appropriate treatment for SUI. | Strong |
4.2.4.3.2. Surgery for women with uncomplicated stress urinary incontinence
The principal procedures evaluated are:
- open and laparoscopic colposuspension;
- autologous “traditional” slings;
- bulking agents;
- synthetic MUS.
4.2.4.3.2.1. Open- and laparoscopic colposuspension surgery
Open Burch colposuspension was previously considered the most appropriate surgical intervention for SUI, and was used as the comparator in RCTs of newer, less-invasive surgical techniques. These include laparoscopic techniques, which have enabled colposuspension to be performed with a minimally-invasive approach.
Open colposuspension
A number of SRs have covered open surgery for SUI, with a large number of RCTs [359,361-364]. The Cochrane review on open colposuspension [364] included 55 trials comprising 5,417 women. In most of these trials, open Burch colposuspension was used as the comparator to an experimental procedure. Within the first year, complete continence rates of 85–90% were achieved for open colposuspension, while failure rates in terms of recurrent UI were 17% up to five years and 21% at > 5 years. The risk of reoperation after Burch colposuspension is estimated at 6% within five years [77] and 10.8% within nine years [365]. The reoperation rate specifically for UI was only 2%. Burch colposuspension was associated with a higher rate of development of enterocoele/vault/cervical prolapse (42%) and rectocele (49%) at five years compared to TVT (23% and 32%, respectively). The rate of cystocoele was similar after Burch colposuspension (37%) and after TVT (41%). The Cochrane review concluded that open colposuspension is an effective treatment for SUI and around 70% of women can expect to be dry at five years after surgery.
Laparoscopic colposuspension
A Cochrane review reported on twelve trials comparing laparoscopic to open Burch colposuspension [362]. Although these procedures had a similar subjective cure rate, there was limited evidence suggesting the objective outcomes were poorer for laparoscopic colposuspension. The ESTER SR [359], based on a network meta-analysis, showed that at twelve months open colposuspension was more effective than laparoscopic colposuspension (nine trials) but these findings were based on low-quality evidence. The Surface Under the Cumulative Ranking (SUCRA) score, which is a numerical representation of the overall performance of the treatment, and represents a single number associated with each intervention, was 76.7% after open colposuspension and 48.9% after laparoscopic colposuspension. Laparoscopic colposuspension had a shorter duration and subsequent hospital stay and may be slightly more cost-effective when compared with open colposuspension after 24 months’ follow-up.
Single-port laparoscopic Burch can be an alternative treatment, although data confirming efficacy are limited [366].
Complications
Voiding difficulties are more common after laparoscopic colposuspension than after retropubic MUS (7.5% vs. 5.1%) [359]. There was no difference between open colposuspension and retropubic MUS (7.8% vs. 7.5%; OR: 0.87) [359]. The results for the comparisons of de novo symptoms of urgency or UUI between open colposuspension and retropubic MUS (11% vs. 8%, OR: 1.49) did not favour either treatment and showed wide confidence intervals [359]. The rate of bladder or urethral perforation was higher for laparoscopic colposuspension compared with open colposuspension (3.7% vs. 0.7%; OR: 4.65) [359].
4.2.4.3.2.1.1.Summary of evidence and recommendation for open and laparoscopic colposuspension surgery
Summary of evidence | LE |
High subjective cure rates are associated with both open and laparoscopic colposuspension for treatment of SUI. | 1a |
Objective cure rates are higher for open compared to laparoscopic colposuspension. | 1a |
Colposuspension is associated with a higher long-term risk of POP than MUS. | 1a |
Laparoscopic colposuspension has a shorter hospital stay and may be more cost-effective than open colposuspension. | 1a |
Laparoscopic colposuspension is associated with higher rates of intraoperative bladder perforation and postoperative voiding dysfunction compared to open colposuspension. | 1a |
The rates of de novo urinary urgency following colposuspension are similar to other surgical treatments for SUI. | 1a |
Recommendation | Strength rating |
Offer colposuspension (open or laparoscopic) to women seeking surgical treatment for SUI following a thorough discussion of the risks and benefits relative to other surgical modalities. | Strong |
4.2.4.3.2.2. Autologous sling
In the past, autologous, cadaveric, xenograft, and synthetic materials have been used for bladder neck pubovaginal sling. Nowadays, use of autologous tissue, either rectus sheath or fascia lata, is the most studied material with the strongest evidence base to support its use [367]. The ESTER SR included three trials of autologous sling vs. open colposuspension, six trials of autologous sling vs. retropubic MUS and one trial of autologous sling vs. transobturator MUS. The quality of evidence was overall very low. The pooled estimate showed that fascial sling had a higher cure rate at one year than open colposuspension (OR: 1.24), retropubic MUS (OR: 1.06) and transobturator MUS (OR: 1.44) but without significance. The SUCRA score was 89.4% for women cured after autologous fascial sling. A sub-analysis from a Cochrane review showed autologous slings had better effectiveness compared to colposuspension at one to five years’ follow-up [364]. In an RCT of Burch colposuspension vs. autologous slings, complete continence rates decreased substantially over time in both arms. At five years, the continence rate of colposuspension was 24.1% compared to 30.8% for fascial slings. Satisfaction remained higher in the sling group (83% vs. 73%) and was directly related to continence
status [368].
Complications
Adverse events rates were similar for the two treatment groups (Burch 10% and sling 9%) although postoperative obstruction was found exclusively in the sling group. Voiding difficulties appear to be more common after autologous sling (15.4% vs. 10.2%; OR: 1.46) than after retropubic MUS. Compared with open colposuspension, the rate of bladder or urethral perforation was lower for traditional sling (0.6% vs. 3.0%; OR:0.20) [359].
4.2.4.3.2.2.1.Summary of evidence and recommendation for autologous sling
Summary of evidence | LE |
High cure rates are associated with autologous sling placement for treatment of SUI. | 1a |
Autologous sling is more effective in terms of cure rate than colposuspension. | 1a |
Autologous sling has a similar rate of adverse events compared to open colposuspension, with higher rates of voiding dysfunction and postoperative UTI, but lower rates of POP and bladder or urethral perforation. | 1a |
Recommendation | Strength rating |
Offer autologous sling placement to women seeking surgical treatment for stress urinary incontinence following a thorough discussion of the risks and benefits relative to other surgical modalities. | Strong |
4.2.4.3.2.3. Urethral bulking agents
The concept of this procedure originates from the idea that intra- or peri-urethral injection of an agent able to form artificial cushions under/around the urethra increases resistance at the bladder outlet and facilitates continence.
In a Cochrane SR [369], 2,004 patients were included from fourteen trials of seven different types of intraurethral injection: Ethylene vinyl alcohol copolymer (Uryx™), glutaraldehyde cross-linked collagen (Contigent©), a porcine dermal implant (Permacol©), solid silicone elastomer (Macroplastique©), autologous fat, pyrolytic carbon (Durasphere©), calcium hydroxylapatite (Coaptite©), Polytetrafluoroethylene (Polytef™) and hyaluronic with dextran polymer (Zuidex©). The conclusions state that the available evidence base remains insufficient to guide practice [369].
A recent SR of 56 studies conclude that available data support the use of Bulkamid® and Macroplastique®, which have shown a short-term efficacy of 30%–90% and 40%–85%, respectively, and long-term efficacy of 42%–70%, and 21%–80%, respectively. Bulkamid® appears to have a more favourable safety profile, with no cases of erosion or migration of product associated with its use. Direct comparisons of urethral bulking agents were not performed [370].
A SR of 23 studies using Macroplastique© including 958 patients showed a 75% improvement with 43% dry rate at < 6 months and a 64% improvement and 36% cure rate at > 18 months [371]. A review of 514 elderly women with SUI treated with various agents showed a reduced pad weight in 73% at one-year follow-up, independent of the material injected [372]. The heterogeneity of the populations, the variety of materials used and the lack of long-term follow-up limit guidance for practice. Most of the studies showed a tendency for short-term improvement in UI, with the exception of one RCT, which did not find a difference between saline and fat injection [373].
One trial of 30 women showed a weak, non-significant advantage in terms of patient satisfaction after mid-urethral injection in comparison to bladder neck injection but with no demonstrable difference in continence levels [369]. One small trial found 30% (six out of 20) of patients developed retention of urine following peri-urethral injection compared with 5% (one out of 20) with transurethral injection [374]. A small RCT found no difference in efficacy between mid-urethral and bladder neck injection of collagen [375]. One study treated patients who had received radiotherapy with injection of Bulkamid® and reported ~25% cure at short-term follow-up [376].
Bulking agent injection is generally safe, and the most frequent adverse event is UTI. However, autologous fat or hyaluronic acid should not be used due to the risk of fatal embolism and local abscess formation, respectively [373,377].
A study reported that women treated by a high-volume surgeon (defined > 75 urethral bulking injections performed over surgical career) had an increased chance of cure and a lower risk of hospital contact postoperatively, compared with women treated by a low-volume surgeon. The risk of 30-day hospital contact was also lower for women treated in a high-volume department (defined > 15 procedures performed per year) [378].
Comparison with other surgical procedures
Two RCTs compared collagen injection to conventional surgery for SUI (silicon particles vs. autologous sling and collagen vs. other surgical procedures). The studies reported greater efficacy but higher complication rates for open surgery [379,380].
In a recent non-inferiority clinical trial, women with primary SUI were randomised to TVT or polyacrylamide hydrogel urethral bulking agent injection (Bulkamid®) [381]. Mid-urethral TVT slings were associated with better satisfaction and cure rates than Bulkamid® in primary SUI. For objective cure rate, the cough stress test was negative in 95.0% of patients who underwent TVT vs. 66.4% who underwent Bulkamid®.
Another SR examining the relative efficacy of urethral bulking agents [382] included six studies in the quantitative synthesis for a total of 710 patients. The authors found that bulking agents are less effective than other surgical procedures according to subjective improvement after treatment (relative risk [RR] = 0.70; 95% CI: 0.53-0.92). However, the main limitation of this SR and meta-analysis was the absence of a common objective outcome measure to evaluate effectiveness.
4.2.4.3.2.3.1.Summary of evidence and recommendations for urethral bulking agents
Summary of evidence | LE |
Urethral bulking agents may provide short-term improvement and cure in women with SUI. | 1b |
Bulking agents are less effective than MUS, Burch colposuspension or autologous sling for cure of SUI and repeat injections may be required in order to achieve sustained benefits. | 1b |
Autologous fat and hyaluronic acid as bulking agents have a higher risk of adverse events. | 1a |
Adverse event rates for urethral bulking agents are lower compared to open surgery. | 2a |
There is no evidence that one type of bulking agent is better than another. | 1b |
The peri-urethral route of injection of bulking agents may be associated with a higher risk of urinary retention compared to the transurethral route. | 2b |
Recommendations | Strength rating |
Offer urethral bulking agents to women seeking surgical treatment for stress urinary incontinence (SUI) following a thorough discussion of the risks and benefits relative to other surgical modalities. | Strong |
Offer urethral bulking agents to women with SUI who request a low-risk procedure with the understanding that efficacy is lower than other surgical procedures, repeat injections are likely, and long-term durability and safety are not established. | Strong |
Do not offer autologous fat and hyaluronic acid as urethral bulking agents due to the higher risk of adverse events. | Strong |
4.2.4.3.2.4. Laser treatment
A SR including sixteen published studies, involving 899 patients with SUI, evaluated effects of laser treatment. The change in the ICIQ-SF score at one, two, and six months was -5.49, -4.97, and -5.48, respectively. The improvement in a 1-hour pad weight test results at one, three-, and twelve-months post treatment was -5.59, -4.96, and -5.82, respectively. The Pelvic organ prolapse/UI sexual questionnaire (PISQ-12) score increased by 5.39 (95% CI: 1.20-9.58) following treatment. Subgroup analysis identified the type and severity of UI as the potential source of heterogeneity. Adverse effects were reported in six of the sixteen trials and affected only a small number of patients. Most adverse events were mild or moderate and required no medical intervention or resolved in a few days. According to this SR, vaginal laser therapy appears to be a safe, effective, and minimally-invasive treatment option for SUI that can be well tolerated by patients [383].
Another SR including 31 studies and 1,530 women confirmed that laser therapy seems to have a beneficial effect on prolapse and UI, but the level of evidence remains low without any suggestion on the laser type to be used, furthermore no studies are available on cost-effectiveness, in particular looking at a longer-term perspective, because surgical results may have more longevity than laser treatment, which may require re-application [384].
Another SR including a total of 27 studies, evaluated the effects of Er:YAG and Fractional CO2 lasers. The overall quality of studies was poor, and 23/27 studies were case series (LE:4). Er:YAG laser showed a modest reduction in mild SUI cases, with benefits lasting a maximum of thirteen to sixteen months. Fractional CO2 laser showed an improvement of mild SUI in few studies; however, no long-term data are available. When reported, adverse events were insignificant, however, they were not reported systematically [260]. A randomised double-blinded sham-controlled study in women with SUI [385] showed a significant reduction in the ICIQ-UI-SF after Er:YAG laser therapy vs. sham manipulated. However, only 21% were subjectively dry (ICIQ-SF = 0) vs. 4% of sham-operated women.
Overall, several limitations have been noted in the current literature regarding vaginal lasers, including variation in laser settings and protocols, short term follow-up, lack of urodynamic evaluation, and poor reporting of appropriate objective measures and adverse events. Based on the available literature, lasers cannot currently be recommended as a treatment option for SUI.
4.2.4.3.2.4.1.Summary of evidence and recommendations for laser treatment
Summary of evidence | LE |
Several limitations have been noted in the current literature regarding vaginal laser treatment for SUI. These include variation in laser settings and protocols, short term follow-up, lack of urodynamic evaluation, and poor reporting of appropriate objective measures and adverse events. | 1b |
Recommendations | Strength rating |
Do not offer vaginal laser therapy to treat stress urinary incontinence symptoms outside of a well-regulated clinical research trial. | Strong |
4.2.4.3.2.5. Mid-urethral slings
Early clinical studies identified that non-autologous synthetic slings should be made from monofilament, nonabsorbable material, typically polypropylene, constructed as a 1–2 cm-wide mesh with a large pore size (macroporous) and coloured to facilitate removal [386]. Mid-urethral slings are now the most frequently used surgical intervention in Europe for women with SUI.
Transobturator route versus retropubic route
A Cochrane meta-analysis of MUS procedures for SUI in women was performed in 2017, spanning January 1947 to June 2014 [387]. Moderate-quality evidence from 55 studies showed variable, but comparable, subjective cure rates between retropubic (71–97%) and transobturator (62–98%) slings in the short term (up to one year). No difference in the objective cure rate in the short term was found. However, the ESTER SR [359], based on a network meta-analysis including 36 trials of overall moderate quality, showed that at twelve months retropubic MUS was more effective than transobturator MUS (OR: 0.74). The SUCRA scores for women cured after retropubic MUS were 89.1% vs. 64.1% after transobturator MUS. However, there was no significant difference in these cure rates between the two approaches. Similarly, based on 40 moderate-quality trials, retropubic MUS performed better than the transobturator approach in terms of symptom improvement
(RR: 0.76) but the difference was, again, not significant.
Analysis of a randomised equivalence trial of retropubic vs. transobturator MUS for the treatment of SUI in women shows similar findings. This trial confirms equivalence of objective cure rates at twelve but not at 24 months (77.3% and 72.3% objective cure rate for retropubic and transobturator surgery). For both types of MUS, subjective and objective treatment success decreased over time and equivalence of the retropubic and the transobturator routes could not be confirmed at 24 and 60 months, with retropubic MUS demonstrating an increased benefit, despite satisfaction remaining high in both arms [388]. Five years after surgical treatment, objective success was 7.9% greater in women assigned to retropubic sling compared to transobturator sling (51.3% vs. 43.4%), not meeting prespecified criteria for equivalence. Patient satisfaction decreased over five years but remained high and similar between treatment arms (retropubic sling 79% vs. transobturator sling 85%) [389].
In terms of long-term complications, data are scant but in one study de novo OAB developed in 14% of patients at ten years post transobturator tension-free vaginal tape (TVT-O) [390]. In a multicentre prospective study of women undergoing TOT, failure of previous anti-incontinence procedures was the only predictor of recurrence of SUI [390].
A long-term cohort study of retropubic TVT showed an 89.9% objective cure rate and a 76.1% subjective cure rate at ten years. Overall, 82.6% of patients reported high satisfaction with surgery [391]. A long-term prospective study on transobturator sling showed that, at 145 months, the objective and subjective cure rates were 78.9% and 62.6%, respectively; with no significant deterioration in SUI cure rates over time [392]. Another long-term follow-up study of patients treated with TVT showed a sustained response with 95.3%, 97.6%, 97.0% and 87.2% of patients being cured or improved at five, seven, eleven and seventeen years, respectively [393]. The ESTER network meta-analysis based on cure and improvement suggested that, when comparing surgical treatments for SUI, retropubic MUS, transobturator MUS and traditional sling had the highest efficacy, but this ranking does not consider the complication profile of these techniques. The short- to medium-term adverse event data are sparse [359].
Several health economic analyses of MUS procedures have been published with conflicting results. In a review of 26 economic evaluations and on the basis of a cost–utility and value of information analysis over a ten-year period, the authors concluded that MUS remains among the most cost-effective approaches [360]. A primary economic evaluation of retropubic vs. transobturator tapes over a five-year time period suggested that the latter may be cost-effective and cost-saving compared to the standard TVT approach [394]. Conversely, the findings from the ESTER network meta-analysis stated that over a lifetime, retropubic MUS was, on average, the least costly and most effective surgery but the level of uncertainty in these analyses was high.
Insertion using a skin-to-vagina direction versus a vagina-to-skin direction
The Cochrane review on MUS for female SUI showed no difference in the short- and medium-term subjective cure rates in vagina-to-skin (inside-out) vs. skin-to-vagina (outside-in) approaches, based on moderate-quality evidence [395]. Voiding dysfunction seems to be more frequent in the vagina-to-skin (inside-out) transobturator tape (TOT) group, but this approach is associated with a lower frequency of vaginal perforations (RR: 0.25). Due to the low quality of the evidence, it is unclear whether the lower frequency of vaginal perforations with this approach is responsible for the lower rate of vaginal tape erosions. Likewise, a meta-analysis of RCTs demonstrated no significant difference in efficacy between outside-in and inside-out approaches, but vaginal perforations were, again, less frequent in the latter group (2.6% vs. 11.8%, OR: 0.21) [396]. The five-year data of a prospective, non-RCT of the two techniques showed a high objective success rate (82.6 vs. 82.5%, respectively) with no difference between the two approaches [397]. In a secondary analysis of the E-TOT study (a study of transobturator MUS in the treatment of women with urodynamic MUI), no difference in the patient-reported success rates was found between the vagina-to-skin (inside-out) and the skin-to-vagina (outside-in) groups (63.2% and 65.5%, respectively; OR: 1.11) at nine years follow-up [398].
Complications of synthetic mid-urethral slings
The ESTER network meta-analysis noted that comparative assessment of adverse events between different procedures was not always possible due to the lack of available data [359]. Direct comparisons using head-to-head meta-analyses were mainly carried out for retropubic MUS, transobturator MUS or single-incision slings. The authors did, however, comment that “For other intervention comparisons, the number of studies was generally small and the CIs wide. However, there was some evidence to suggest that bladder perforation was more likely to occur after retropubic MUS than after transobturator MUS, open colposuspension or traditional sling”. In particular, the retropubic approach for MUS was associated with a significantly higher rate of bladder perforation than transobturator MUS was (5% vs. 0.2%). Regarding de novo voiding dysfunction, 36 studies compared transobturator MUS with retropubic MUS, favouring the former (OR: 0.51). For pain, it is worth noting that it was defined and measured in many different ways across individual trials and across Cochrane reviews. Some pain outcomes were categorised by location (e.g., suprapubic) or time (e.g., short, or long term). These discrepancies made it difficult to combine data from different studies. Data were available mainly for the comparison between retropubic and transobturator MUS and other surgical procedures. However, groin pain was more frequent after transobturator MUS than retropubic MUS (6.3% vs. 1.3%; OR: 3.80). Converse findings were reported for suprapubic pain, which was higher following TVT (1.2% vs. 4.0%; OR: 0.37). Visceral injury (0.5% vs. 2.4% OR: 0.36), mean operating time, intraoperative blood loss and hospital stay were lower in the transobturator than retropubic MUS groups. The overall vaginal erosion risk was low and comparable in both groups [359].
The rate of tape/mesh exposure or extrusion between retropubic and transobturator MUS was similar (2.1% vs. 2.4%; OR: 1.10). The exact time points at which measurements occurred could not be derived from the Cochrane reviews but most studies were reported to have a short follow-up period (< 12 months), with only a few studies having > 2 years’ follow-up [359]. Repeat surgery for UI was more common in the transobturator group (RR = 8.79); however, the data are limited and of low quality.
A population-based study performed in Scotland in > 16,000 women with SUI showed a similar rate of complications between mesh and non-mesh surgery [399]. However, a recent study of > 92,000 patients followed in the UK National Health Service showed a significant (9.8%) rate of complications using a broader definition and following patients for a longer period [400]. The level of detail regarding the precise nature of complications in this paper was poor. These findings suggest that, as with any SUI surgery, MUS can be associated with complications and fully informed consent is mandatory.
In general, the available published evidence would suggest that MUS does not seem to be associated with significantly higher rates of morbidity and complications compared to other surgeries for SUI, such as open retropubic Burch colposuspension. Pelvic organ prolapse is more common after colposuspension while voiding dysfunction occurs more often after MUS [364]. The ESTER review has commented that the level of detail regarding short-to-medium adverse event data is poor for all SUI surgeries [359] and the Panel is aware of the recent findings from the Independent Medicines and Medical Devices Safety Review in the UK that has raised the possibility that the level of complications from synthetic MUS may be higher than the medical literature would suggest [357].
The ESTER SR included seven studies comparing reintervention after transobturator and retropubic MUS [359]. Pooled analysis of these studies showed wide CIs and considerable uncertainty around the estimated OR (twelve-month post-surgery: 1.37). At one to five years after the procedure, rates of repeat continence surgery were higher in women undergoing transobturator MUS (18.3%) compared with retropubic MUS (0.5%), although only two studies were available for the analysis. A similar trend was observed in studies with a longer follow-up period (> 5 years) but the pooled analysis of these studies showed wide CIs. For retropubic MUS surgery, the bottom-to-top route was 10% more efficacious than top-to-bottom in terms of subjective cure and it was associated with less voiding dysfunction, bladder perforations and vaginal erosion [359].
Single-incision mid-urethral slings
Although there have been many studies published on single-incision devices, it should be noted that there are significant differences in technical design between devices and it may be misleading to make general statements about them as a class of operation. It should also be noted that some devices have been withdrawn from the market (e.g., TVT Secur®, Minitape, MiniArc®), and yet evidence relating to these devices may still be included in current meta-analyses. There is evidence to suggest that single-incision slings are quicker to perform and cause less postoperative thigh pain, but there is no difference in the rate of chronic pain. There is insufficient evidence for direct comparisons between single-incision slings, and no conclusions have been reached about differences between devices.
The ESTER SR showed, based on low-quality evidence, that at twelve months, retropubic and transobturator MUS were more effective than single-incision sling (TVT, OR: 0.50; TOT, OR: 0.68). The SUCRA score was 39.8% for women cured after single-incision slings. However, since not all single-incision devices have been assessed in a comparative RCT, it may be unsafe to assume that they are collectively technically similar or exhibit the same levels of efficacy.
A recent multicentre noninferiority RCT compared single-incision slings (Ajust® and Altis®) with conventional MUS during 36 months of follow-up, defining patient-reported success as a response of very much or much improved in the Patient Global Impression of Improvement questionnaire. After 36 months of follow-up success was reported by 177 of 246 patients (72.0%) and by 157 of 235 patients (66.8%) in the single-incision and MUS group, respectively. The authors conclude that single-incision slings were non-inferior to standard MUS with respect to patient-reported success at fifteen months, and the percentage of patients reporting success remained similar in the two groups at 36-month follow-up [401].
Complications of single-incision slings
Meta-analysis of comparison between single-incision sling and transobturator MUS showed similar rates of mesh erosion or extrusion between interventions (4.8% vs. 3.7%; OR: 1.23). Rates of postoperative pain were higher after retropubic MUS than after single-incision slings (19.2% vs. 6.8%; OR: 0.21).
A non-inferior RCT showed at 36 months a percentage of patients with groin or thigh pain of 14.1% with single-incision slings and 14.9% with MUS. Over the 36-month follow-up period, the percentage of patients with tape or mesh exposure was 3.3% with single-incision slings and 1.9% with MUS, and the percentage who underwent further surgery for SUI was 2.5% and 1.1%, respectively [401]. A multicentre single blind RCT compared postoperative pain scores and efficacy of a single-incision sling (Ajust®, n = 100) and a standard TOT (n = 56). Immediate postoperative pain was significantly lower for single-incision sling group, but de novo dyspareunia was higher (38.5% vs. 25%, with no statistical difference). No differences were reported in the objective cure at twelve months (90% vs. 88%) [402].
The rate of unspecified pain was higher after transobturator MUS than after single-incision sling at twelve months (1.0% vs. 5.2%; OR: 0.24) and 24 months (1.4% vs. 10.4%; OR: 0.16). Single-incision sling was associated with more repeat surgery compared with transobturator MUS (5.1% vs. 2.9%; OR: 1.57). At > 3 years after the procedure, the repeat surgery rate was 10.3% for single-incision slings vs. 7.6% for transobturator MUS (OR: 1.42) [359].
Sexual function after synthetic mid-urethral sling surgery
A SR examining the effect of synthetic MUS on female sexual function suggested different and contradictory results between studies. More studies have shown an improvement, or no change, in sexual function because of a reduction in coital incontinence, anxiety and avoidance of sex. Dyspareunia was the most common cause of worsening of sexual function and the precise incidence is difficult to estimate as many studies did not report it [403]. A meta-analysis of outcome measures in trials of sling procedures suggests that single-incision slings are associated with a significantly higher improvement in sexual function, however conflicting evidence was seen, compared to standard MUS procedures [404]. A recent RCT comparing single-incision slings with MUS showed similar outcomes with respect to QoL and sexual function in the two groups, with the exception of dyspareunia. Among the 290 women responding to a validated questionnaire, dyspareunia was reported by 11.7% in the single-incision group and 4.8% in the MUS group [401].
4.2.4.3.2.5.1.Summary of evidence and recommendations for mid-urethral slings
Summary of evidence | LE |
The retropubic MUS appears to provide better patient-reported subjective and objective cure of SUI, compared with colposuspension. | 1a |
Synthetic MUSs inserted by the transobturator or retropubic route provide equivalent patient-reported outcomes at one year. | 1a |
Synthetic MUSs inserted by the retropubic route have higher patient-reported cure rates in the longer term. | 1b |
Long-term analyses of MUS cohorts showed a sustained response beyond 10 years. | 2b |
The retropubic route of insertion, compared with the transobturator route, is associated with a higher intraoperative risk of bladder perforation and a higher rate of voiding dysfunction. | 1a |
The transobturator route of insertion is associated with a higher risk of groin pain than the retropubic route. | 1a |
Long-term analysis of MUS showed no difference in terms of efficacy for the skin-to-vagina (outside-in) compared to vagina-to-skin (inside-out) directions up to nine years. | 2a |
The top-to-bottom (inside-out) direction in the retropubic approach is associated with a higher risk of postoperative voiding dysfunction. | 1b |
The comparative efficacy of Ajust® and Altis® single-incision slings against conventional MUS at fifteen and 36 months is non-inferior. | 1b |
Operating times for insertion of single-incision MUSs are shorter than for standard retropubic slings. | 1b |
Blood loss and immediate postoperative pain are lower for insertion of single-incision slings compared with conventional MUS. | 1b |
The rate of mesh exposure, repeat SUI surgery and dyspareunia at 3 years is higher for single-incision slings (Ajust® and Alits®) compared to conventional MUS. | 1b |
There is no evidence that other adverse outcomes from surgery are more or less likely with single-incision slings than with conventional MUS. | 1b |
In women undergoing surgery for SUI, coital incontinence is likely to improve. | 3 |
Overall, there is conflicting evidence regarding sexual function following SUI surgery. | 1a |
NB: Most evidence on single-incision slings is from studies using the tension-free vaginal tape secure device,and although this device is no longer available, it is, however, still included in many systematic reviews and meta-analyses.
Recommendations | Strength rating |
Offer a mid-urethral sling (MUS) to women seeking surgical treatment for stress urinary incontinence following a thorough discussion of the risks and benefits relative to other surgical modalities. | Strong |
Inform women that long-term outcomes from MUS inserted by the retropubic route are superior to those inserted via the transobturator route. | Strong |
Inform women of the complications associated with MUS procedures and discuss all alternative treatments in the light of recent publicity surrounding surgical mesh. | Strong |
Inform women who are being offered single-incision slings (Ajust® and Altis®), that short term efficacy appears equivalent compared to conventional MUS. | Strong |
Inform women who are being offered a single-incision sling that long-term efficacy remains uncertain. | Strong |
4.2.4.3.2.6. Other treatments for uncomplicated stress urinary incontinence
Intravesical balloon treatment has been explored for women with SUI. The Vesair® gas-filled intravesical balloon differs from other treatment methods in that it is not intended to increase outlet resistance or minimise urethral hypermobility but to attenuate the fluctuation of intravesical pressure when the abdominal pressure increases [405,406]. Two sham controlled RCTs have evaluated the Vesair® intravesical balloon [405,407]. Both reported significant reductions in incontinence symptoms and pad weight, but QoL was not significantly different between study arms. High levels of adverse events were reported in both trials as well as significant numbers of withdrawals/device removals. The most common adverse events were dysuria, urgency, gross haematuria and UTIs.
Mechanical devices have been used to treat SUI for centuries. There are several devices available which act either by supporting the bladder neck or urethra to address urethral hypermobility, or by occluding the urethral lumen. A Cochrane review of eight RCTs that included three small trials comparing mechanical devices to no treatment found inconclusive evidence of benefit [408]. Another SR of mechanical devices concluded that there was insufficient evidence to support their use in women [409]. The place of mechanical devices in the management of SUI remains in question. Currently, there is little evidence from controlled trials on which to judge whether their use is better than no treatment, and large well-conducted trials are required for clarification. There is also insufficient evidence in favour of one particular device and few comparisons of mechanical devices with other forms of treatment [408].
Systematic reviews support the use of compression devices such as the adjustable compression therapy and artificial urinary sphincter (AUS) devices [410,411]. Although these procedures are largely reserved for those with recurrent or complicated SUI (see Section 4.2.4.3.3.3 External compression devices), these recent additions to the literature include the use of some compression devices for uncomplicated SUI.
4.2.4.3.2.6.1.Summary of evidence and recommendations for other treatments for uncomplicated stress urinary incontinence
Summary of evidence | LE |
Implantation of an artificial sphincter can improve or cure incontinence in women with uncomplicated SUI. | 3 |
Implantation of the adjustable compression therapy (ACT®) device may improve uncomplicated SUI. | 3 |
Complications, mechanical failure and device explantation often occur with both the artificial sphincter and ACT©. | 3 |
Recommendations | Strength rating |
Offer mechanical devices to women with mild-to-moderate SUI who fail conservative treatment only as part of a well-conducted research trial. | Strong |
Inform women receiving artificial urinary sphincter or adjustable compression device (ACT®) that, although cure is possible, even in expert centres there is a high risk of complications, mechanical failure, or a need for explantation. | Strong |
4.2.4.3.3. Surgery for women with complicated stress urinary incontinence
This section addresses surgical treatment for women with complicated SUI as defined in Section 4.2.2.
Women with associated genitourinary prolapse are included in Section 4.7.
The principal procedures included are:
- Colposuspension or MUS (synthetic or autologous) following failed primary SUI surgery;
- External compression devices: adjustable compression therapy (ACT®) and AUS;
- Adjustable slings.
4.2.4.3.3.1. Colposuspension or mid-urethral sling (synthetic or autologous) following failed primary stress urinary incontinence surgery
Urinary incontinence following SUI surgery may indicate persistent or recurrent SUI, or the development of de novo UUI, or both. Careful evaluation including urodynamics is an essential part of the work-up of these patients.
Most of the data on surgery for SUI refer to primary operations. Even when secondary procedures have been included, it is unusual for the outcomes in this subgroup to be separately reported. When they are, the numbers of patients are usually too small to allow meaningful comparisons. This means that no firm recommendations can be made regarding which modality is best for the treatment of recurrent SUI, and previous SRs have commented that in view of the absence of any evidence, clinicians must rely largely on expert opinion or personal experience when advising patients about treatment options [412].
The ESTER network meta-analysis revealed that women with transobturator MUS were more likely to undergo repeat surgery than those who had retropubic MUS, and fewer repeat operations were observed after retropubic MUS compared with other interventions [359]. A recent update of two Urinary Incontinence Treatment Network trials [413] compared the retreatment-free survival rates by initial surgical procedure. Five-year retreatment-free survival rates were 87%, 96%, 97%, and 99% for Burch colposuspension, autologous fascial sling, transobturator, and retropubic MUS, respectively. Types of surgical retreatment included autologous fascial sling (19), bulking agent (18), and synthetic sling (1). This suggests that MUS may not be preferred in cases of recurrent SUI [413].
In these cohorts, 6% of women after standard anti-incontinence procedures were retreated within five years, mostly with injection therapy or autologous fascial sling. Not all women with recurrent SUI chose surgical retreatment.
A Cochrane review attempted to summarise the data regarding different types of MUS procedures for recurrent SUI after failure of primary surgical therapy [414]. The literature search identified 58 records, but all were excluded from quantitative analysis because they did not meet eligibility criteria. Overall, there were no data to recommend or refute any of the different management strategies for recurrent or persistent SUI after failed MUS surgery. Another SR looking at the effectiveness of MUS in recurrent SUI included twelve studies and reported an overall subjective cure rate following MUS for recurrent SUI after any previous surgery of 78.5% at an average 29 months’ follow-up [415]. The subjective cure rate following MUS after previous failed MUS was 73.3% at follow-up of sixteen months. The authors commented that there was a lower cure rate with transobturator compared to the retropubic tape for recurrent SUI after previous surgery. Conflicting evidence comes from a SR assessing the effectiveness and complications of various surgical procedures for female recurrent SUI and reported on data from 350 women in ten RCTs with a mean follow-up of 18.1 months [416]. The authors found no difference in patient-reported and objective cure/improvement rates between retropubic and transobturator MUS in the setting of recurrent SUI. There was also no significant difference between Burch colposuspension and retropubic MUS in terms of patient-reported improvement or objective cure/improvement.
A SR of older trials of open surgery for SUI suggested that the longer-term outcomes of repeat open Burch colposuspension may be poor compared to autologous fascial slings [417]. Similarly, one large non-randomised comparative series suggested that cure rates after more than two previous operations were 0% for open Burch colposuspension and 38% for autologous fascial sling [418].
4.2.4.3.3.1.1.Summary of evidence for surgery in those with recurrent stress urinary incontinence following failed primary surgery
Summary of evidence | LE |
Failure rates of single-incision slings appear higher than with other types of MUS. | 1a |
The incidence of repeat surgery is higher in those women who underwent primary transobturator compared to retropubic MUS. | 1a |
The five-year failure rate of Burch colposuspension appears higher than for synthetic or traditional sling procedures. | 2b |
Some studies suggest that retropubic synthetic MUS procedures appear to be more effective than transobturator MUS for the treatment of recurrent SUI, but this is not a consistent finding in the literature. | 1a |
Most procedures are less effective when used as second-line procedures. | 2a |
Burch colposuspension has similar short-term patient-reported or objective cure rates when compared to TVT for treatment of recurrent SUI. | 1b |
Autologous sling appears superior to Burch colposuspension for treatment of recurrent SUI. | 2b |
4.2.4.3.3.2. Adjustable slings
Although adjustable slings are most commonly used for treatment of complicated SUI, they may also be considered for uncomplicated SUI. There are no RCTs investigating outcome of adjustable sling insertion for women with SUI. There are limited data from cohort studies on adjustable tension slings with variable selection criteria and outcome definitions. Few studies have included sufficient numbers of patients or have long enough follow-up to provide useful evidence.
One adjustable sling is the Remeex system (Neomedic International®, Terrassa, Spain), which was investigated in a prospective study of 230 women with SUI [419]. After a mean follow-up of 89 months, 165 patients were cured of SUI (71.7% in the intention-to-treat [ITT] analysis, 80.5% in per protocol [PP] analysis). Forty patients remained incontinent (17.4% in ITT, 19.5% in PP) and 88 patients required readjustment of the sling during follow-up.
The tension was increased in 82 cases due to recurrence of SUI and reduced in six due to outlet obstruction. The currently available adjustable sling devices have differing designs, making it difficult to draw general conclusions about them as a class of procedure.
4.2.4.3.3.2.1.Summary of evidence for adjustable slings
Summary of evidence | LE |
There is only low-level evidence to suggest that adjustable MUS devices may be effective for cure or improvement of SUI in women. | 3 |
There is no evidence that adjustable slings are superior to standard MUS. | 4 |
4.2.4.3.3.3. External compression devices
External compression devices are usually used for treatment of recurrent SUI after failure of previous surgery but can be considered for primary treatment. Studies have largely included patients with profound intrinsic failure of the sphincter mechanism, characterised by low VLPP or urethral closure pressure [410,411]. The two intracorporeal external urethral compression devices available are the adjustable compression therapy (ACT®) device and AUS.
ACT®: Using US or fluoroscopic guidance, the ACT® device is inserted by placement of two inflatable spherical balloons; one on either side of the bladder neck. The volume of each balloon can be adjusted through a subcutaneous port placed within the labia majora. A SR including eight studies published between 2007 and 2013 with follow-up of one to six years revealed 15–44% of patients considered that their SUI had been cured and 66–78.4% were satisfied [410]. The explantation rate was 19–31%. In these studies, a significant reduction in the number of pads used daily was consistently observed after ACT® balloon placement and QoL was significantly improved. The authors concluded that ACT® balloons constitute a reasonable, minimally-invasive alternative for treatment of female SUI due to intrinsic sphincter deficiency, especially in patients who have already experienced failure of standard surgical treatment.
AUS: The major advantage of AUS over other anti-incontinence procedures is the perceived ability to be able to void normally [408]. There have been a few case series of AUS in women, with populations of 45–215 patients and follow-up of one month to 25 years [420-423]. Case series have been confounded by varying selection criteria, especially the proportion of women who have neurological dysfunction or who have had previous surgery. Most patients achieved an improvement in SUI, with reported subjective cure in 59–88%. Common adverse effects included mechanical failure requiring revision (< 42% at ten years) and explantation (5.9–15%). In a retrospective series of 215 women followed-up for a mean six years, the risk factors for failure were older age, previous Burch colposuspension and pelvic radiotherapy [423].
Early reports of laparoscopically implanted AUS do not have sufficient patient populations or sufficient follow-up to be able to draw any conclusions [424,425].
A more recent SR included seventeen studies, but all were retrospective or prospective non-comparative case series [411]. Most patients had undergone at least one anti-incontinence surgical procedure prior to AUS implantation (69.1–100%). Outcomes revealed that complete continence rates were 61–100%. The rates of explantation were 0–45%, erosion rates were 0–22% and mechanical failure rates were 0–44%. The authors concluded that AUS can provide excellent functional outcomes in women with SUI resulting from intrinsic urethral sphincter deficiency but at the cost of high morbidity.
4.2.4.3.3.3.1.Summary of evidence for external compression devices
Summary of evidence | LE |
Implantation of an artificial sphincter improves or cures incontinence in women with SUI caused by sphincter insufficiency. | 3 |
Implantation of the AUS device may improve complicated SUI. | 3 |
Implantation of the ACT® device may improve complicated SUI. | 3 |
Complications, mechanical failure, and device explantation often occur with both the artificial sphincter and ACT®. | 3 |
Explantation of AUS is more frequent in older women and among those who have had previous Burch colposuspension or pelvic radiotherapy. | 3 |
4.2.4.3.3.4. Recommendations for complicated stress urinary incontinence
Recommendations | Strength rating |
Management of complicated stress urinary incontinence (SUI) should only be offered in centres with appropriate experience (see Section: 4.2.4.3.1). | Strong |
Base the choice of surgery for recurrent SUI on careful evaluation, including individual patient factors and considering further investigations such as cystoscopy, multichannel urodynamics, as appropriate. | Strong |
Inform women with recurrent SUI that the outcome of a surgical procedure, when used as second-line treatment, is generally inferior to its use as first-line treatment, both in terms of reduced efficacy and increased risk of complications. | Weak |
Only offer adjustable mid-urethral sling as primary surgical treatment for SUI as part of a structured research programme. | Strong |
Consider secondary synthetic sling, bulking agents, Burch colposuspension, autologous sling or artificial urinary sphincter (AUS) as options for women with complicated SUI. | Weak |
Inform women receiving AUS or ACT® device that, although cure is possible, even in expert centres, there is a high risk of complications, mechanical failure, or a need for explantation. | Strong |
4.2.4.3.4. Surgery for stress urinary incontinence in special patient groups
4.2.4.3.4.1. Stress urinary incontinence surgery in obese women
There is no agreement about the outcome of incontinence surgery in obese women. Secondary analysis of an RCT on retropubic and transobturator tapes for treatment of women with SUI suggests that obese women experience inferior outcome compared to non-obese women. Stratification of patients according to BMI (< 30 and > 30) shows a significant difference in objective dry rates (negative pad test) at one year (85.6% vs. 67.8%) and five years (87.4% vs. 65.9%) and subjective cure (absence of SUI symptoms) at one year (85.8% vs. 70.7%) and five years (76.7% vs. 53.6%). At one and five years, 6.7% and 16.3% of patients who were initially dry (negative pad test) after surgery developed a positive pad test [426,427].
Conversely, short-term outcome of single-incision MiniArc® sling showed comparable objective cure rates (negative cough stress test) at two years (86% and 81% in non-obese and obese women, respectively); similar improvement of the Urinary Distress Inventory six and Incontinence Impact Questionnaire seven was observed in non-obese and obese women [428]. Objective cure rate was also similar with Altis® (88% and 87% in non-obese and obese women) at two years follow-up [429].
4.2.4.3.4.2. Stress urinary incontinence surgery in elderly women
Age appears to be a significant factor in outcome from SUI surgery but there is conflicting evidence. An RCT of 537 women comparing retropubic to transobturator tape, showed that increasing age was an independent risk factor for failure of surgery over the age of 50 years [430]. An RCT assessing risk factors for the failure of TVT vs. TVT-O in 162 women also found that age was a specific risk factor for recurrence at one year [431]. In addition, based on a sub-analysis of a trial cohort of 655 women at two years’ follow-up, it was shown that elderly women were more likely to have a positive stress test at follow-up, were less likely to report objective or subjective improvement in stress and UUI, and were more likely to undergo retreatment for SUI. There was no difference in time to postoperative normal voiding [432].
Another RCT comparing immediate TVT vs. no surgery (or delayed TVT) in older women, confirmed efficacy of surgery in terms of QoL and satisfaction, but with more complications in the surgical arm [433].
Furthermore, a SR of the efficacy of treatments of UI in older patients suggests that MUS is successful in older patients (> 65 years) with 5.2–17.6% reporting persistent SUI after surgery. No difference in the frequency of de novo UUI, persistent UUI or persistent SUI was found in older patients [361].
4.2.4.3.4.3. Summary of evidence and recommendations for stress urinary incontinence surgery in special patient groups
Summary of evidence | LE |
Incontinence surgery may be safely performed in obese women; however, outcomes may be inferior. | 1 |
The risk of failure from surgical repair of SUI, and the risk of adverse events, appears to increase with age. | 2b |
There is no evidence that any surgical procedure has greater efficacy or safety in older women than another procedure. | 4 |
Recommendations | Strength rating |
Inform obese women with stress urinary incontinence (SUI) about the increased risks associated with surgery, together with the lower probability of benefit. | Weak |
Inform older women with SUI about the increased risks associated with surgery, together with the likelihood of lower probability of benefit. | Weak |
4.2.5. Follow-up
The follow-up of patients with SUI is dependent on the treatment given. For conservative and physical therapies, sufficient time should be allowed for the demonstration of a therapeutic effect. For pharmacological treatment, early follow-up is recommended. For most surgical interventions, short-term follow-up should be arranged to assess efficacy and identify any early postoperative complications.
The Panel is supportive of long-term outcome assessment via registries and recognises the paucity of high-quality long-term data, specifically regarding complications from surgery.
4.3. Mixed urinary incontinence
The term MUI is broad because it may refer to equal stress and urgency symptoms, stress-predominant symptoms, urgency-predominant symptoms, urodynamic stress urinary incontinence (USUI or USI) with DO or USUI with clinical urgency symptoms, but no DO [434]. The challenge of this broad definition is that it leads to inconsistencies when evaluating treatment options and outcomes.
4.3.1. Epidemiology, aetiology and pathophysiology
The prevalence rates of MUI vary widely in the literature. Most epidemiological studies have either not considered subtypes of UI, or only reported on SUI, UUI and MUI. The current literature is unclear regarding the population prevalence and risks for the different UI subtypes [435]. There are many urinary symptom questionnaires used in epidemiological research, with varying evidence of validity. Caution is needed when comparing epidemiological studies that do or do not report a separate MUI subgroup, and when generalising from population level data to clinical practice. The problems arise from significant heterogeneity in terms of types of questionnaires/surveys used, population parameters, variable response rates, varying definitions of MUI, and outcome measures.
It seems apparent, however, that MUI is the second most common form of UI, after SUI, with most studies reporting a 7.5–25% prevalence [435]. One can extrapolate that among women with UI, approximately one-third have MUI [436]. In a secondary analysis of a large clinical trial, 655 women were evaluated for UI and their response to treatment [437]. It was found that 50−90% of women fell into the category of MUI based on patient-reported answers to the Medical Epidemiologic and Social Aspects of Aging and Urinary Distress Inventory (UDI) questionnaires. However, when objective criteria such as urodynamic findings were used, only 8% of women were categorised as having MUI.
Mixed urinary incontinence is usually caused by a combination of the same factors that cause SUI and UUI. Several factors may be responsible for its development, including oestrogen deficiency, abnormalities in histomorphology, and microstructural changes [438]. One report postulates that an incompetent sphincter and bladder neck allow urine to enter the proximal urethra during stress, causing a urethro-detrusor reflex that triggers involuntary detrusor contraction, which then causes urgency and UUI [439]. Another study has shown that urine flow across the urethral mucosa increases the excitability of the micturition reflex [440]. Ultimately, it is unlikely that one theory or risk factor can explain the development of MUI and its symptoms; it is more probable that disturbances in several elements and the lack of bladder compensation results in the development of MUI [438].
4.3.2. Diagnostic evaluation
Assessment of patients with MUI begins with a thorough history of the patient’s urinary symptoms and follows the recommendations set out in the general evaluation and diagnosis of LUTS in Chapter 3. It is conventional to try and categorise MUI as either stress or urge predominant.
Mixed urinary incontinence is difficult to diagnose, as the condition comprises many phenotypes. Some women exhibit detrusor contractions provoked by physical stressors, some have unprovoked detrusor contractions, and many have no abnormal detrusor contractions, but still report urine leakage with the sensation of urgency. Some women with urgency symptoms do not manifest UUI because their urethral sphincter is strong and often able to prevent urine leakage [441].
The role of urodynamics in MUI is unclear but establishing objective degrees of SUI and DO incontinence may help in counselling patients about the most appropriate initial treatment option.
4.3.2.1. Summary of evidence and recommendations for the diagnosis of mixed urinary incontinence
Summary of evidence | LE |
There is no evidence that urodynamics affects outcomes of treatment for MUI. | 3 |
Recommendations | Strength rating |
Complete a thorough history and examination as part of the assessment of mixed urinary incontinence (MUI). | Strong |
Characterise MUI as either stress-predominant or urgency-predominant where possible. | Weak |
Use bladder diaries and urodynamics as part of the multimodal assessment of MUI to help inform the most appropriate management strategy. | Strong |
4.3.3. Disease management
4.3.3.1. Conservative management
Women with MUI generally have more severe symptoms and respond less well to treatment than women with only SUI or UUI [442]. Clinicians are encouraged to begin treatment for MUI with conservative management directed toward the most bothersome component of the symptom spectrum and to reserve surgery as a last resort [441].
4.3.3.1.1. Pelvic floor muscle training
An RCT comparing PFMT with and without an audiotape for 71 women with UI did not find any difference between the two treatment arms [443]. Mean number of incontinent episodes per day decreased from 3.9 overall to 3.2 for participants with MUI. Six months after completing the course of exercises, approximately one third of all enrolees reported that they continued to note good or excellent improvement and desired no further treatment.
A small RCT including 34 women with SUI and MUI compared eight weeks of PFMT with no treatment and found that PFMT significantly increased PFM strength, improving QoL, and reduced the frequency of UI episodes compared to no treatment [444]. Another RCT including SUI and MUI confirmed these results [445].
A multicentre randomised controlled non-inferiority trial on 467 women with MUI was conducted in ten hospitals. Participants were randomised 1:1 to receive EA (36 sessions over twelve weeks with 24 weeks of follow-up) or PFMT–solifenacin (5 mg/day) over 36 weeks. In women with moderate-to-severe MUI, EA was not inferior to PFMT–solifenacin in decreasing the 72-hour incontinence episodes (between-group difference, –1.34%) [446].
In a comparative study of the effectiveness of behavioural therapy and PFMT (combined with MUS vs. sling alone in women with MUI), 416 (86.7%) had post-baseline outcome data and were included in the primary twelve-month analyses [447]. The UDI score in both groups significantly decreased (178.0 to 30.7 points in the combined group, 176.8 to 34.5 points in the sling-only group). The model estimated between-group difference, did not meet the minimal clinically important difference threshold. Adherence to the behavioural therapy and PFMT regimes, which is a prerequisite for achieving a satisfactory outcome, was not reported in the study.
A Cochrane review comparing PFMT with no or sham treatment included 31 RCTs from fourteen countries, but there was only one study including women with MUI and one with UUI and none of them reported data on cure, improvement, or number of episodes of these subgroups [316].
The effect of combining biofeedback with PFMT has already been fully addressed in Section 4.2.4.1.3, and there was no evidence of any additional benefit in a population with predominantly MUI.
4.3.3.1.2. Bladder training
Details on BT programmes are given in Section 4.2.4. The ICI 2017 [322] concluded that for women with UUI or MUI, PFMT and BT are effective first-line conservative therapies. One RCT assigned 108 women with diagnoses of SUI (n = 50), UUI (n = 16), or MUI (n = 42) to six weeks of BT and PFMT or BT alone [448]. Overall, and in the SUI and MUI subgroups, significantly more patients in the BT and PFMT group reported cure and improved symptoms.
4.3.3.1.3. Electrical stimulation
A Cochrane review on ES for SUI included participants with SUI or stress-predominant MUI. Twenty-five percent of the included trials were deemed to have a high risk of bias due to a variety of factors, including baseline differences between groups and industry funding. For subjective cure or improvement of SUI, low-quality evidence indicated that ES was better than no active treatment or sham treatment. Electrical stimulation for OAB and SUI is covered in Sections 4.1.4.1.5.4 and 4.2.4.1.3.2.
4.3.3.2. Summary of evidence and recommendations for conservative management in mixed urinary incontinence
Summary of evidence | LE |
Pelvic floor muscle training appears less effective for MUI than for SUI alone. | 2 |
Pelvic floor muscle training is better than no treatment for improving UI and QoL in women with MUI. | 1a |
Bladder training combined with PFMT may be beneficial in the treatment of MUI. | 1b |
Recommendations | Strength rating |
Treat the most bothersome symptom first in patients with mixed urinary incontinence (MUI). | Weak |
Offer bladder training as a first-line therapy to adults with MUI. | Strong |
Offer supervised intensive pelvic floor muscle training, lasting at least three months, as a first-line therapy to all women with MUI (including elderly and postnatal women). | Strong |
4.3.3.3. Pharmacological management
Many RCTs include patients with MUI with predominant symptoms of either SUI or UUI but few report outcomes separately for those with MUI compared to pure SUI or UUI groups.
4.3.3.3.1. Anticholinergics
In an RCT of 854 women with MUI, tolterodine ER was effective for improvement of UUI but not SUI, suggesting that the efficacy of tolterodine for UUI was not altered by the presence of SUI [449]. In another study (n = 1,380) tolterodine was equally effective in reducing urgency and UUI symptoms, regardless of whether there was associated SUI [450]. Similar results were found for solifenacin [451,452].
4.3.3.3.2. Duloxetine
In one RCT of duloxetine vs. placebo, 588 women were stratified into either stress-predominant, urgency-predominant or balanced MUI groups. Duloxetine was effective for improvement of incontinence and QoL in all subgroups, although results in the stress-predominant groups were better [453]. Treatment-emergent adverse event rate in the duloxetine group was 61.3% with discontinuation rates of 15.7%. Adverse event rates were higher in those participants taking other concomitant antidepressant agents.
Duloxetine was found to have equal efficacy for SUI and MUI in an RCT (n = 553) following secondary analysis of respective subpopulations, but no adverse events data were reported [454].
4.3.3.3.3. Summary of evidence and recommendations for pharmacological management of mixed urinary incontinence
Summary of evidence | LE |
Limited evidence suggests that anticholinergic drugs are effective for improvement of the UUI component in patients with MUI. | 2 |
Duloxetine is effective for improvement of both SUI and MUI symptoms, but adverse event rates are high. | 1b |
Recommendations | Strength rating |
Treat the most bothersome symptom first in patients with mixed urinary incontinence (MUI). | Weak |
Offer anticholinergic drugs or beta-3 agonists to patients with urgency-predominant MUI. | Strong |
Offer duloxetine (where licensed) to selected patients with stress-predominant MUI unresponsive to other conservative treatments and who want to avoid invasive treatment, counselling carefully about the risk of adverse events. | Weak |
4.3.3.4. Surgical management
The surgical treatment options for MUI, include all the anti-incontinence procedures as outlined in the SUI Section 4.2.4.3.
Many RCTs include patients with pure SUI or pure UUI as well as patients with MUI. However, few RCTs report separate outcomes for MUI subgroups.
Post hoc analysis of a large RCT showed that in women undergoing either autologous fascial sling or Burch colposuspension, the outcomes were poorer for women with a concomitant complaint of preoperative urgency [432]. A similar post hoc review of another RCT comparing transobturator and retropubic MUS showed that the greater the severity of preoperative urgency, the more likely that treatment would fail [98]. However, an earlier study had found that surgery provided similar outcomes, whether or not urgency was present prior to surgery (this study included only a few patients with urodynamic DO). Another RCT including 93 patients with MUI showed a significant improvement in continence and QoL in the group that had TVT and botulinum toxin A (Botox®) rather than with either treatment alone [455].
In a secondary analysis of a study of transobturator TVTs in the treatment of women with urodynamic MUI, no difference in patient-reported success rates was found between the vagina-to-skin (inside-out) and the skin-to vagina (outside-in) groups (63.2% and 65.5%, respectively) at nine years’ follow-up [398].
Analysis of the trial populations included in the meta-analysis on single-incision slings suggests that the evidence can be generalised to women who have predominantly SUI, and no other clinically severe LUT dysfunction. The evidence is not adequate to guide choice of surgical treatment for those women with MUI, severe POP, or a history of previous surgery for SUI.
Research trials should define accurately what is meant by MUI. There is a need for well-designed trials comparing treatments in populations with MUI, and in which the type of MUI has been accurately defined.
4.3.3.4.1. Summary of evidence and recommendations for surgery in patients with mixed urinary incontinence
Summary of evidence | LE |
Women with MUI are less likely to be cured of their UI by SUI surgery than women with SUI alone. | 2 |
The response of pre-existing urgency symptoms to SUI surgery is unpredictable. | 1b |
Recommendations | Strength rating |
Treat the most bothersome symptom first in patients with mixed urinary incontinence (MUI). | Weak |
Warn women that surgery for MUI is less likely to be successful than surgery for stress urinary incontinence alone. | Strong |
Inform women with MUI that one single treatment may not cure urinary incontinence; it may be necessary to treat other components of the incontinence problem as well as the most bothersome symptom. | Weak |
4.4. Underactive bladder
Underactive bladder is a common clinical entity, defined by the ICS as “a symptom complex characterised by a slow urinary stream, hesitancy, and straining to void, with or without a feeling of incomplete bladder emptying sometimes with storage symptoms” [456]. Diagnosis of UAB is based on clinical symptoms and the presentation and aetiology can be variable.
This differs from DU, which is a diagnosis based on urodynamic studies. Detrusor underactivity is defined by the ICS as “a detrusor contraction of reduced strength and/or duration, resulting in prolonged bladder emptying and/or failure to achieve complete bladder emptying within a normal time span” [1]. Acontractile detrusor is specified when there is no measurable detrusor contraction.
Female voiding dysfunction is defined by the ICS as “a diagnosis based on symptoms and urodynamic investigations characterised by abnormally slow and/or incomplete micturition, based on abnormally slow urine flow rates and/or abnormally high PVR volume” [113]; ideally on repeated measurement to confirm abnormality. Pressure–flow studies may be required to determine the precise cause of the voiding dysfunction [31].
4.4.1. Epidemiology, aetiology, pathophysiology
4.4.1.1. Epidemiology
Underactive bladder as an entity remains difficult to characterise, partly because its corresponding urodynamic correlate, DU, remains loosely defined, leading to significant variability in diagnostic criteria across research studies and significant overlap of symptoms with other conditions. As a consequence of the variable definition, reported prevalence also varies and ranges from 12-45% in women, with increased prevalence seen with age [75] and in institutionalised elderly women [457].
Several studies have demonstrated similar prevalence rates for DU in the ambulatory setting of around
12–19% [458-460]. As would be expected, voiding symptoms consistent with UAB are higher. In a large cross-sectional, population-based internet survey conducted in the USA, UK and Sweden including 15,861 women aged > 40 years, 20.1% had weak flow, 27.4% had incomplete bladder emptying and 38.3% had terminal dribbling [5].
Both DO during filling and DU in the voiding phase of urodynamic studies can co-exist (formerly known as detrusor hyperactivity with impaired contractility [DHIC]) and one study showed the prevalence of this finding was over 30% in elderly women [457].
4.4.1.2. Aetiology
The presence of DU in diverse clinical groups suggests multifactorial aetiology [461]. Idiopathic DU is probably partly an age-dependent decrease in detrusor contractility with no other identifiable causes, but young women can also have DU. There are many secondary causes of DU, including neurogenic (e.g., multiple sclerosis, multiple systemic atrophy, spinal cord injury, spina bifida, Parkinson’s disease, hydrocephalus, transverse myelitis, stroke, Guillain–Barré syndrome, diabetes mellitus, and pelvic nerve injury), myogenic (prolonged bladder overdistension, diabetes mellitus, and BOO) and iatrogenic (pelvic surgery) causes [462].
4.4.1.3. Pathophysiology
Many pathways are involved in normal detrusor contraction, and there are different possible sites of dysfunction [75] with a variety of mechanisms involved in UAB (see Figure 1):
- Central circuits and centres (prefrontal cortex, periaqueductal gray, pontine micturition centre and hypothalamus): failure of integration or processing.
- Efferent pathways (sacral cord, sacral nerves, pelvic nerves, and postganglionic neurons): impaired detrusor activation.
- Afferent pathways (peripheral afferent nerves, anterolateral white column, and posterior column): early termination of voiding reflex.
- Muscle (detrusor myocytes and extracellular matrix): loss of intrinsic contractility.
Different aetiologies can share common pathophysiological mechanisms: for example, diabetes mellitus affects mainly afferent pathways and the detrusor muscle; and neurogenic diseases affect central circuits and efferent/afferent pathways.
Figure 1: Management and treatment of women presenting with urinary incontinence, site of dysfunction, major aetiological factors, mechanisms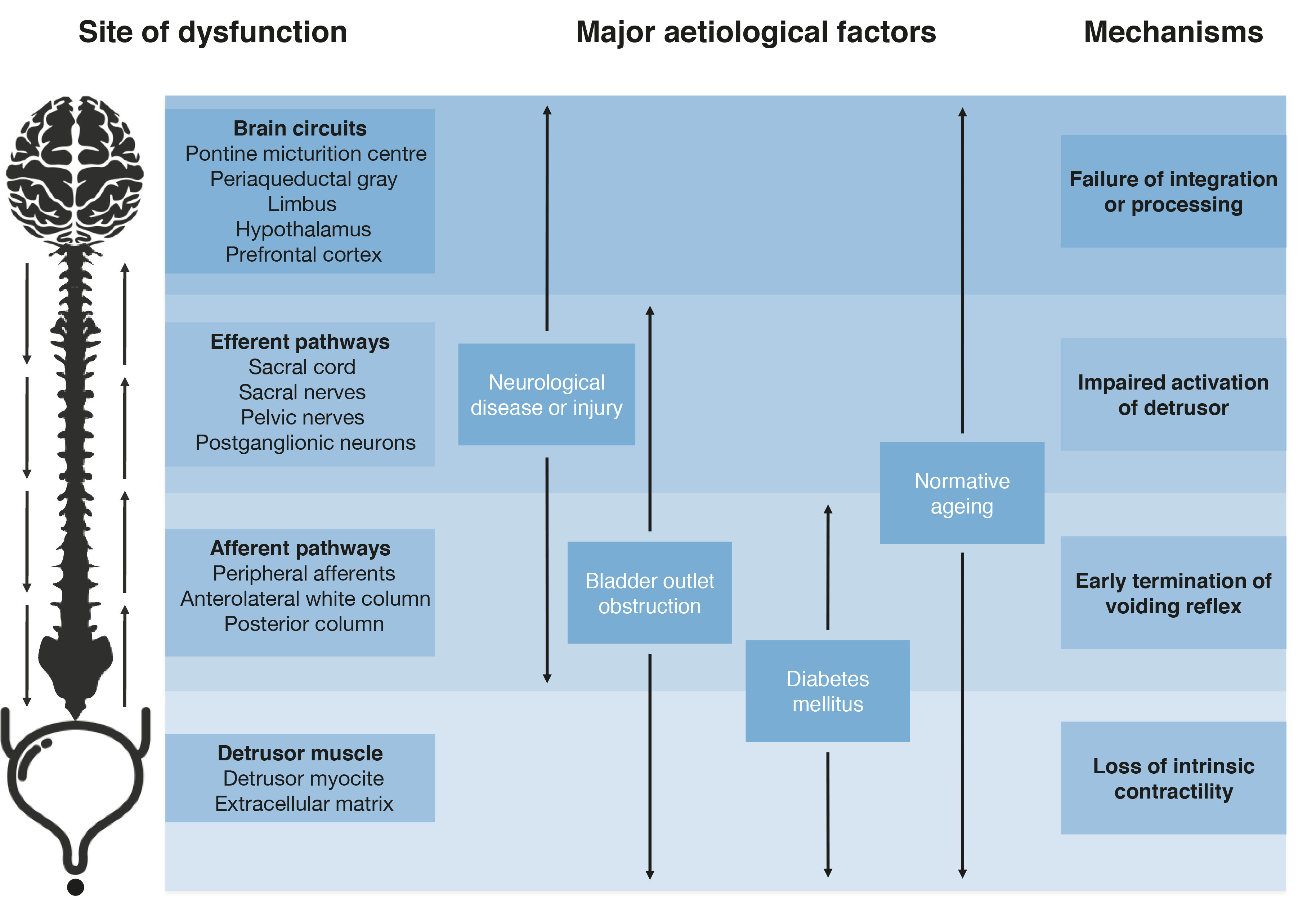 *Figure reproduced with permission from the publisher, from Osman N. et al. [785]
*Figure reproduced with permission from the publisher, from Osman N. et al. [785]
4.4.2. Classification
There is no current classification system of UAB. Patients can be classified according to presumed aetiology or pathogenic mechanism, but without sufficient longitudinal data or high-level evidence to establish prognostic factors, the classification of UAB patients in terms of relevant clinical characteristics or risk of complications is not possible.
4.4.3. Diagnostic evaluation
4.4.3.1. Symptoms associated with detrusor underactivity
A retrospective study correlated LUTS with urodynamic findings in 1,788 patients (1,281 women). Women with DU, defined as detrusor pressure at maximum flow rate (PdetQmax) < 20 cm H2O, maximum flow rate (Qmax) < 15 mL/s, BVE < 90% and no sign of obstruction on video-urodynamic studies, had a significantly higher occurrence of reduced and/or interrupted stream, hesitancy, feeling of incomplete bladder emptying, palpable bladder, and absent and/or decreased sensation compared with women with normal pressure and flow [463]. A qualitative study on a small sample of male and female patients diagnosed with DU reported a variety of LUTS and associated impact on QoL. Storage symptoms of nocturia, increased daytime frequency, and urgency, and the voiding symptoms of slow stream, hesitancy, and straining were reported by over half of the patients. A sensation of incomplete emptying and post-micturition dribble were also frequently described. The impact of their symptoms on QoL was variable, but in general, storage symptoms were more bothersome [464].
Based on current data, it is not possible to find a pivotal symptom or collection of symptoms to identify DU patients. The ICI Questionnaire-Underactive Bladder (ICIQ-UAB) has been developed as a research PROM tool [465].
4.4.3.2. Urodynamic studies
Non-invasive studies like uroflowmetry, PVR volume measurement and BVE determination are potentially useful to identify women who might have DU. There is considerable symptomatic overlap with BOO, and uroflowmetry and PVR volume findings may also be similar. Only invasive urodynamics with pressure–flow studies can reliably distinguish DU from BOO and these urodynamic diagnoses can coexist. Diagnosis in women is particularly difficult as they can void by relaxing the pelvic floor, that is, without detectable detrusor contraction during pressure–flow study and without increased abdominal pressure [466]. The simplest methods to define and diagnose DU are based on the use of cut-off values of Qmax and PdetQmax, possibly combined with cut-off values of PVR volume and BVE. However, there is no consensus on which cut-off values should be used [467]. It is obvious that the prevalence of DU depends on the criteria used. In a retrospective study of 1,015 women, DU was found in 14.9% when using Qmax < 12 mL/s or PVR volume > 150 mL; in 9.6% when using PdetQmax < 30 cm H2O and Qmax < 10 mL/s; and in 6.4% when using PdetQmax < 20 cm H2O, Qmax < 15 mL/s and BVE < 90% [468].
More elaborate methods combine urodynamic data into an index or a physical quantity that reflects bladder contraction strength. A value below a certain threshold would thus diagnose DU. Again, there is no consensus regarding what is normal/abnormal. Table 4 provides an overview of the best-known parameters, their background, and typical values. Watt’s factor (WF) estimates the power generated by the detrusor per unit area of bladder surface [469] and it varies during voiding. Usually, WFmax is considered. Alternatively, its value at Qmax can be used. Projected isovolumetric pressure (PIP) is a gross simplification of the bladder output relation and estimates the maximum detrusor pressure that can be generated by the bladder when the outlet is closed; the isovolumetric detrusor pressure. The bladder contractility index (BCI) is a reduction of PIP to an index [470]. The population in which PIP and BCI were developed mainly consisted of men. Projected isovolumetric pressure 1, is similar to PIP and also estimates the isovolumetric detrusor pressure, but was developed in an entirely female population via an experimental method [471].
A third method of quantifying bladder contraction strength involves stop tests. One study compared three types of direct measurement of isovolumetric pressure: (1) the voluntary stop test, in which the patient voluntarily interrupted flow; (2) the mechanical stop test, in which flow was interrupted by a balloon catheter; and (3) the continuous occlusion test, in which the subject tried to void against a blocked outlet. The latter had the best reliability and best detected drug-induced changes, though the results of the mechanical stop tests were
similar [472].
All parameters discussed above give some information about the strength of detrusor contraction in a given void. They do not necessarily reflect what the detrusor might potentially achieve under optimum conditions [473]. Also, they give no information on voiding duration. No parameters for this are available. Finally, abnormally low bladder contraction strength does not necessarily imply insufficient bladder contraction strength to achieve optimal voiding. Table 4 summarises different parameters to measure detrusor contraction in female patients.
Table 4: Most used parameters to measure detrusor contraction in female patients
Parameter | Basis | Population | Values |
Watt’s factor [469] | Hill equation of muscle contraction in a spherical organ, with fixed constants obtained from experimental and clinical studies | Eight asymptomatic female volunteers aged 28–45 years (median 34 years) | Ideal voiding (bell-shaped flow curves): WFmax 11-24 W/m2 Non-ideal voiding: WFmax Normally WFmax > 7 W/m2 (expert opinion, unspecified population) [474] |
Projected isovolumetric pressure (cm H2O) and BCI, using PIP as an index [470,475] | Bladder output relation, simplified to a straight line with fixed slope of | Unspecified population, mainly men with BPO | Classification based on expert opinion: > 150: strong contraction 100–150: normal contraction 50–100: weak contraction < 50: very weak contraction |
Projected isovolumetric pressure 1 (cm H2O) [471] | Comparison of Qmax and PdetQmax values with stop test results (Formula: pdetQmax + Qmax) | 100 women with UUI aged 53–89 (mean 70) years | 5th-95th percentile: 29–78 cm H2O Mean: 49 cm H2O Median: 48 cm H2O Proposed typical values: 30-75 cm H2O |
Continuous occlusion test [472] | Direct measurement of isovolumetric voiding contraction | 70 women with UUI aged 53–89 (mean: 70) years | Mean ± SD: 48.7 ± 24.4 cm H2O |
BCI = Bladder contractility index; PIP = Projected isovolumetric pressure; UUI = urgency urinary incontinence;WF = Watt’s factor.
4.4.4. Disease management
As there are different possible causes and pathogenic mechanisms involved in female UAB, preventive and therapeutic strategies are difficult to define. Among preventive strategies, early recognition after major surgery or labour might prevent long-term problems associated with prolonged bladder over-distension. Nerve-sparing techniques for radical pelvic surgery are more favourable in terms of early recovery of bladder function [476,477].
Treatment of female DU includes strategies to ensure bladder drainage, increase bladder contraction, decrease urethral resistance, or a combination of the two [474]. The management goals for UAB are to improve symptoms and QoL, to reduce the risk of complications, and to identify situations where interventions may not be appropriate.
4.4.4.1. Conservative management
4.4.4.1.1. Behavioural interventions
Regular or timed voiding in women with impaired bladder sensations have been done to avoid bladder over-distention. Assisted voiding by abdominal straining with adequate relaxation of the PFM, double or triple voiding are potential strategies to improve bladder emptying. However, none of these manoeuvres has proven efficacy in an RCT. Furthermore, there is a possible association between voiding by excessive abdominal straining and the risk of POP [478]. A small retrospective study in women with neurogenic acontractile detrusor secondary to spina bifida showed that Valsalva voiding may increase the risk of rectal prolapse compared with CISC [479].
4.4.4.1.2. Pelvic floor muscle relaxation training with biofeedback
There are no RCTs on PFM relaxation training in adult women with UAB. Contrary to common beliefs, one study found significant relaxation of the PFMs after contraction [480] and another study found that PFM relaxation training over time increased the speed of relaxation after a single contraction [481]. There is some evidence from the paediatric literature, including one RCT that compared efficacy of PFM relaxation with biofeedback plus combined therapy (including hydration, scheduled voiding, toilet training and diet) vs. combined therapy alone in children with non-neuropathic UAB and voiding dysfunction. Mean number of voiding episodes was significantly increased in the relaxation training group compared with the group with only combined treatment. Post-void residual volume and voiding time decreased considerably, whereas maximum urine flow increased significantly in the relaxation group compared with the combined treatment group [482].
4.4.4.1.3. Clean intermittent self-catheterisation
Clean intermittent self-catheterisation is the most commonly used therapy to manage high PVR volume and urinary retention [117]. It reduces the risk of complications such as UTI, UUT deterioration, bladder stones and overflow UI, etc. It has not yet been established whether the incidence of UTI, other complications and user satisfaction, are affected by either sterile or clean intermittent catheterisation (IC), coated or uncoated catheters or by any other strategy [483]. The use of hydrophilic catheters may be associated with a lower rate of UTI, but further evidence is needed, as current data comes from neurogenic patients [484]. The average frequency of catheterisation is four to six times per day [485] and the catheter sizes most often used are 12–16 Fr. In aseptic IC, an optimum frequency of five times showed a reduction of UTI [485]. Frequency of catheterisation needs to be based on individual need and capability, to prevent chronic and repeated over-filling of the bladder [486]. Thorough counselling regarding techniques, frequency, equipment, and adverse effects of CISC should be given to all potential patients in line with good medical practice.
For people using CISC, a Cochrane review found no evidence that one type of catheter or regimen of catheterisation was better than another [487]. However, a recent narrative review suggests that, in certain populations, single-use catheters may reduce urethral trauma and UTI [488].
4.4.4.1.4. Indwelling catheter
Indwelling urinary catheter may be an option for some women who have failed all other treatments and are unable to perform CISC. Complications include UTI, stone formation, and urethral damage. Suprapubic catheterisation may be preferable over urethral catheterisation to minimise the risk of urethral trauma and pain [489].
4.4.4.1.5. Intravesical electrical stimulation
Intravesical electrical stimulation (IVES) can be used to improve bladder dysfunction by stimulating A-delta mechanoreceptor afferents but requires intact afferent circuits and healthy detrusor muscle. One retrospective study in sixteen patients (eleven females) found that two-thirds of patients with a weak detrusor after prolonged bladder over-distension regained balanced voiding after IVES due to detrusor reinforcement [490].
4.4.4.2. Pharmacological management
4.4.4.2.1. Parasympathomimetics
Theoretical approaches to UAB pharmacological treatment include direct stimulation of detrusor cell muscarinic receptors using parasympathomimetic agents such as carbachol or bethanechol or acetylcholinesterase inhibitors such as distigmine, pyridostigmine or neostigmine.
A SR on the use of parasympathomimetics in patients with UAB included ten RCTs (controls typically received placebo or no treatment). Three studies reported significant improvements relative to the control group, but six did not and one even reported significant worsening of symptoms. There was no evidence for differences between individual drugs, specific uses of such drugs, or in outcome measures [491]. The review concluded that the available studies do not support the use of parasympathomimetic for treating UAB, especially when frequent and/or serious adverse effects (gastrointestinal upset, blurred vision, bronchospasm, and bradycardia) are taken into account.
4.4.4.2.2. Alpha-adrenergic blockers
In order to improve bladder emptying, decreasing outlet resistance through sympathetic blockade at the bladder neck/urethra has been investigated. One prospective study with tamsulosin showed similar improvement in terms of uroflowmetry parameters (specifically in the percentage of patients who had a good therapeutic response) in women with BOO (39.4%) or DU (32.7%) [492]. Another longitudinal study including fourteen women with DU showed clinical and urodynamic improvements after tamsulosin [493]. A prospective single-blind RCT in female patients with DU compared the efficacy of alpha-blocker, cholinergic drugs, or combination therapy, with the latter exhibiting the best results [494].
4.4.4.2.3. Prostaglandins
Prostaglandins are prokinetic agents that promote smooth muscle contraction. Prostaglandins E2 and F2 have been used intravesically to treat urinary retention after surgery. A Cochrane review showed a significant association between intravesical prostaglandin and successful voiding among postoperative patients with urinary retention. However, the success rate was low (32%) with wide 95% CI, compared to placebo. The RCTs included in the pooled analysis were underpowered with methodological limitations and the event rate was very low, indicating a very low certainty of the evidence [495]. Intravesical prostaglandin treatment is rarely used, and further research is necessary before it can be taken up more widely.
4.4.4.3. Surgical management
4.4.4.3.1. Sacral nerve stimulation
Sacral nerve stimulation is often used for therapy of non-obstructive urinary retention. The mechanism of action has not been fully elucidated, but activation of afferent sensory pathways, modulation–activation of the central nervous system, and inhibition of inappropriate activation of the guarding reflex are some of the mechanisms proposed.
An RCT included 37 patients in the implantation arm and 31 in the standard medical therapy arm, showing a mean decrease in PVR volume and a mean increase in voided PVR volume compared to standard treatment [496]. A meta-analysis of seven studies also showed a mean difference in PVR volume reduction of 236 mL and a mean voided volume increase of 299 mL [497]. The response rate during the trial phase ranged from 33-90% (mean 54.2%) and the success rate of permanent implantation ranged from 55-100% (mean 73.9%), highlighting that patient selection is crucial [498].
The importance of careful patient selection has been emphasised with one study suggesting women with evidence of anatomical BOO, suspected loss of intrinsic detrusor contractility or neurogenic bladder dysfunction show lower response rates [499].
4.4.4.3.2. Onabotulinumtoxin A
OnabotulinumtoxinA intersphincteric injections in external striated urethral sphincter may improve voiding in patients with DU by reducing outlet resistance and reducing the guarding reflex. Some retrospective case studies have shown improvement in voiding symptoms, recovery of spontaneous voiding, and improvement in urodynamic parameters (reduction of voiding pressure and/or urethral closure pressures, reduced PVR volume) [500,501]. The duration of symptomatic relief is short; typically, three months but the reported incidence of de novo SUI is low.
4.4.4.3.3. Transurethral incision of the bladder neck
Transurethral incision of the bladder neck has been described in a small series of women with refractory DU. In a retrospective case study, 40/82 (48.8%) women achieved satisfactory outcomes (spontaneous voiding with voiding efficiency > 50%), but five (6.1%) patients developed SUI and two (2.4%) developed a vesico-vaginal fistula [502].
4.4.4.3.4. Myoplasty
One retrospective multicentre study reported the long-term results of latissimus dorsi detrusor myoplasty in patients with bladder acontractility, with 71% recovering complete spontaneous voiding, with a mean PVR volume of 25 mL [503]. No other groups have published their experience to reproduce these findings.
4.4.4.4. Summary of therapeutic evidence on detrusor underactivity
The level of evidence for most therapeutic interventions for DU is low. Only CISC remains as a gold standard to reduce the adverse consequences of a high PVR volume and incomplete voiding, in spite of the low level of evidence that supports this statement.
4.4.4.4.1. Summary of evidence and recommendations for underactive bladder
Summary of evidence | LE |
Abdominal straining with relaxation of the PFM may improve bladder emptying but increases the risk of POP. | 3 |
Pelvic floor muscle relaxation training may increase voiding episodes, decrease post-void residual volume and voiding time. | 3 |
Clean intermittent self-catheterisation has proven efficacy in terms of effecting bladder emptying in patients who are unable to do so. | 3 |
Indwelling transurethral catheterisation and suprapubic cystostomy are associated with a range of complications as well as an increased risk of UTI. | 3 |
Intravesical electrical stimulation may be useful in some patients after prolonged bladder over-distension, but long-term efficacy remains unproven. | 3 |
Parasympathomimetics do not improve clinical or urodynamic parameters of UAB and frequent and/or serious adverse effects may arise. | 1b |
Alpha-adrenergic blockers in women with UAB may be effective in improving voided volume and reducing PVR volume. | 2b |
Very low certainty evidence indicates that intravesical prostaglandins may promote successful voiding in patients with urinary retention after surgery. | 1a |
Sacral nerve stimulation improves voided volume and decreases PVR volume in women with DU. | 1b |
There is limited evidence for the effectiveness of onabotulinumtoxinA external urethral sphincter injections to improve voiding in women with UAB. | 3 |
Transurethral bladder neck incision may improve voiding in women with DU, but complications (SUI, vesico-vaginal fistulae) may occur. | 3 |
There is very limited evidence for the effectiveness of detrusor myoplasty for bladder acontractility. | 3 |
Recommendations | Strength rating |
Encourage double voiding in those women who are unable to completely empty their bladder. | Weak |
Warn women with underactive bladder (UAB) who use abdominal straining to improve emptying about pelvic organ prolapse risk. | Weak |
Use clean intermittent self-catheterisation (CISC) as a standard treatment in patients who are unable to empty their bladder. | Strong |
Thoroughly instruct patients in the technique and risks of CISC. | Strong |
Offer indwelling transurethral catheterisation and suprapubic cystostomy only when other modalities for urinary drainage have failed or are unsuitable. | Weak |
Do not routinely recommend intravesical electrical stimulation in women with UAB. | Weak |
Do not routinely recommend parasympathomimetics for treatment of women with UAB. | Strong |
Offer alpha-adrenergic blockers before more-invasive techniques. | Weak |
Offer intravesical prostaglandins to women with urinary retention after surgery only in the context of well-regulated clinical trials. | Weak |
Offer onabotulinumtoxinA external sphincter injections before more-invasive techniques as long as patients are informed that the evidence to support this treatment is of low quality. | Weak |
Offer sacral nerve stimulation to women with UAB refractory to conservative treatment. | Strong |
Do not routinely offer detrusor myoplasty as a treatment for DU. | Weak |
4.4.5. Follow-up
Natural history and clinical evolution at long-term follow-up of women with DU is not well known. No longitudinal cohort studies are described in the literature. The interval between follow-up visits depends on patient characteristics, treatments given and the frequency of urinary complications.
4.5. Bladder outlet obstruction
4.5.1. Introduction
Bladder outlet obstruction is defined by the ICS as “obstruction during voiding, characterised by increased detrusor pressure and reduced urine flow rate” [1]. Its precise diagnosis requires urodynamic evaluation including an assessment of pressure and flow.
Voiding dysfunction has previously been defined in Section 4.4. In women, voiding dysfunction can be caused by BOO or DU [1]. There are also non-obstructive causes and therefore voiding dysfunction, and BOO should not be used interchangeably. Another term that must be differentiated from BOO and voiding dysfunction is dysfunctional voiding, which is a specific and discrete form of voiding dysfunction characterised by an intermittent and/or fluctuating flow rate due to involuntary intermittent contractions of the peri-urethral striated muscle during voiding in neurologically normal individuals [113].
4.5.2. Epidemiology, aetiology, pathophysiology
4.5.2.1. Epidemiology
Estimates of prevalence of BOO among women vary from 2.7-29% [504]. One large series of women undergoing urodynamic evaluation for LUTS found that ~20% are diagnosed with BOO. The wide variance is due to several factors, including differences in definitions and diagnostic criteria for female BOO, differences in study populations, and variation in study methods. The estimated prevalence rates of LUTS due to BOO in women are lower than those reported in men (18.7–18.9% vs. 24.3–24.7%) [505].
Prevalence of voiding LUTS is associated with age [54,506,507], parity [54,508], prolapse [54,508] and prior continence surgery [54,508]. Bladder outlet obstruction has long been postulated to cause mainly voiding symptoms [509] but recent data from a series of 1,142 women referred for evaluation of LUTS suggest that storage symptoms may be predominant in women diagnosed with BOO, and excess daytime urinary frequency was the most common symptom reported by 69% [504].
4.5.2.2. Pathophysiology
Bladder outlet obstruction can be either anatomical (mechanical) or functional. In anatomical BOO, there is a physical or mechanical obstruction to the outflow of urine, whereas in functional BOO there is a non-anatomical, non-neurogenic obstruction of the outlet usually resulting from non-relaxation of the bladder neck, sphincter or PFM, or increased urethral sphincter tone or PFM contraction during voiding, as observed in patients with dysfunctional voiding.
Mechanisms for anatomical (mechanical) obstruction include external compression, fibrosis, stricture or injury to the urethra and kinking of the urethra due to POP. Progressive fibroblastic reaction around the urethra induced by mesh tapes or slings used in incontinence surgery may also cause anatomical (mechanical) obstruction [462]. In a retrospective review of 192 women diagnosed with BOO, 64% had mechanical obstruction [504].
Functional obstruction may be caused by contraction, or failure of relaxation, of the bladder neck and/or urethral sphincter complex or the PFMs during sustained detrusor contraction [509]. The exact causes of this lack of relaxation, or contraction, are often elusive but might be due to sympathetic hyperactivity or hypertrophy of the bladder neck smooth muscle for primary bladder neck obstruction [510], or may be mostly behavioural for dysfunctional voiding [511].
4.5.2.3. Aetiology
Conditions associated with anatomical BOO include POP, incontinence surgery, urethral stricture, urethral stenosis, urethral diverticulum, urethral caruncle, urethral malignancies and paraurethral masses.
Conditions associated with functional BOO include primary bladder neck obstruction, dysfunctional voiding, and idiopathic urinary retention (Fowler’s syndrome).
In primary bladder neck obstruction, the bladder neck fails to open adequately during voiding, in the absence of an anatomical obstruction [512]. It is estimated that 4.6–16% of women presenting with voiding symptoms have primary bladder neck obstruction [510].
Dysfunctional voiding is due to involuntary intermittent contractions of the peri-urethral striated or levator muscles during voiding in neurologically normal women, and is thought to be caused by faulty learned toileting behaviour [462]. There is also some evidence of a link between dysfunctional voiding and a history of sexual abuse [513].
Idiopathic urinary retention, also known as Fowler’s syndrome, is a primary disorder of the external urethral sphincter with hypertrophy of the muscle fibres, which fail to relax during micturition. It is associated with decreased detrusor contractility via enhancement of the guarding reflex. It is seen most often, but not exclusively, in young women with urinary retention and is characterised by increased urinary sphincter volume and activity/tone, which may be hormonally triggered [514].
Alpha-adrenergic agonists, such as pseudoephedrine commonly contained in decongestants, can lead to some form of functional obstruction due to their stimulatory effects, which may contract the bladder neck and lead to urinary retention [515].
Neurological conditions can also bring about functional BOO in women. These conditions are not considered in these guidelines and are covered elsewhere [9].
4.5.3. Classification
4.5.3.1. Anatomic bladder outlet obstruction
Anatomical BOO involves a physical or mechanical obstruction of the outflow of urine not related to urethral or pelvic muscle tone.
4.5.3.2. Functional bladder outlet obstruction
Functional BOO involves a non-anatomical, non-neurogenic obstruction of the outflow of urine resulting from non-relaxation or increased tone in the bladder neck and/or urethral sphincter complex or the PFMs (Table 5). Neurological causes of functional BOO are not considered in these guidelines and are covered in the EAU Guidelines on Neuro-urology [9].
Table 5: Main causes of female bladder outlet obstruction
Functional BOO | Anatomical BOO |
|
|
4.5.3.3. Recommendation for classification of bladder outlet obstruction
Recommendation | Strength rating |
Use standardised classification of bladder outlet obstruction in women (anatomical or functional), and research populations should be fully characterised using such classification. | Strong |
4.5.4. Diagnostic evaluation
Diagnosis of BOO in women, although dependent on formal pressure–flow studies, may be suggested by several clinical and other non-invasive assessments.
4.5.4.1. Clinical history
In terms of clinical history, a range of LUTS may be elicited and these may not be confined to voiding LUTS. Women may not present until they have the possible complications of BOO, such as recurrent UTI, chronic urinary retention or acute/chronic kidney disease [504]. The evidence regarding clinical utility of symptoms for the diagnosis of BOO is inconclusive and limited to small retrospective studies [516,517]. Perhaps some of the difficulty in evaluating the diagnostic accuracy of urinary symptoms comes from the observation that a significant proportion of women presenting with obstruction also have concomitant storage symptoms, making urodynamic evaluation essential. In a large study of > 5,000 women with urinary symptoms including 163 with BOO, additional urodynamic diagnoses were noted in 54% [518].
4.5.4.2. Clinical examination
There are no studies evaluating the clinical utility of physical examination in women with suspected BOO; nevertheless, it is widely considered as a key part of the medical assessment. It allows for visual inspection of the urethra and vagina for possible causes of mechanical obstruction as well as an assessment of the pelvic floor, which may be the cause of functional obstruction.
4.5.4.3. Uroflowmetry and post-void residual volume
Reduced Qmax and incomplete bladder emptying can result from weakness in the contractile strength of the detrusor muscle, or increased outlet resistance due to functional or anatomical/mechanical BOO. The use of uroflowmetry to differentiate between anatomical and functional BOO was explored in a retrospective study of 157 women [511], which concluded that Qmax was significantly lower in patients with anatomical obstruction, but a large degree of overlap was noted. The largest evaluation of the diagnostic utility of urine flow studies and PVR volume estimation was a retrospective analysis of > 1,900 patients with symptoms of voiding dysfunction, of whom > 800 were diagnosed with BOO based on urodynamic assessment [519]. Functional BOO was > 6
times more common than anatomical/mechanical obstruction, which does not agree with most of the other epidemiological literature for female BOO. The authors found that although urine flow rate alone was not accurate enough to diagnose BOO, PVR of > 200 mL could differentiate bladder neck dysfunction from the other causes of BOO, with a receiver-operator characteristics (ROC) area under the curve (AUC) of 0.69. Conversely, in a retrospective study involving 101 women primarily presenting with SUI, a good correlation between abnormal uroflowmetry and urodynamic obstruction (phi = 0.718) was found [520].
4.5.4.4. Ultrasound
The major utility of US scanning in women with BOO is to detect possible complications such as BWT/DWT upper tract dilatation/hydronephrosis. However, the diagnostic capabilities of US have been investigated in a 2021 SR of 16 non-randomised studies and reported a moderate pooled sensitivity and high specificity for DWT, while 6 studies evaluating US-estimated bladder weight (UEBW) reported a high sensitivity and specificity [521]. A prospective case–control study of 27 patients with cystoscopically confirmed bladder neck obstruction [522] reported the diagnostic value of shear wave elastography (SWE) and acoustic radiation force impulse imaging (ARFI) for female BOO was compared and the authors concluded that ARFI was more accurate than SWE, but a combination of the techniques was superior to either one alone.
4.5.4.5. Magnetic resonance imaging
Magnetic resonance imaging in patients with pathological urethral stricture can determine the degree of peri-urethral fibrosis, although the prognostic and clinical significance of such a finding has not been established [523].
4.5.4.6. Electromyography
Electromyography (EMG) has been most extensively studied in the subgroup of women with BOO due to idiopathic urinary retention caused by a high-tone non-relaxing sphincter (Fowler’s syndrome). Abnormal urethral EMG activity may be associated with non-relaxation of the striated sphincter, abnormally high urethral pressure, and, through an exaggerated guarding reflex, poor bladder sensation and reduced detrusor contractile strength [513,524]. Complex repetitive discharges and decelerating bursts are specific urethral EMG abnormalities that have been described in patients with high-tone non-relaxing sphincter, although these abnormalities have also been noted in asymptomatic volunteers [525,526]. A review of voiding dysfunction in women included 65 studies with only a small number addressing the diagnostic utility of PFM EMG [462]. The authors commented that increased EMG activity of the PFM can be seen during voiding or non-relaxation, and when this is coupled with pressure–flow information from urodynamics, it may be useful to differentiate between functional and anatomical obstruction. Further evidence for this comes from a retrospective study of 157 women with roughly equal numbers of women with functional and anatomical obstruction, which concluded that a low level of PFM EMG activity is characteristic of anatomical obstruction [511]. Additional neurophysiological tests, such as anal sphincter EMG, bulbocavernosus reflex, and pudendal sensory evoked potentials can assess the integrity of the somatic S2–4 nerve roots; however, their clinical utility in the context of non-neurogenic female BOO needs to be better defined [513].
4.5.4.7. Cystourethroscopy
Cystourethroscopy can be useful to visualise any anatomical/mechanical obstruction and provide information regarding its nature, location and calibre. Given that pelvic malignancy may cause anatomical BOO, cystourethroscopy is considered an essential part of the diagnostic pathway. Formal urethral calibration may be useful for women with BOO secondary to pathological urethral stricture and various different urethral calibre thresholds have been used, from 14-20 Fr [527].
4.5.4.8. Urodynamics and video-urodynamics
Pressure–flow studies are the mainstay of BOO diagnosis and the characteristic abnormalities are a combination of low flow and concomitant high detrusor pressure [512]. However, while the general definition of BOO is well established, with some data supporting its clinical validity in male patients [528], the urodynamic definition of female BOO remains controversial [509]. Several urodynamic criteria have been introduced but none has been established as a standard due to lack of clinical validation [509,529]. The Blaivas-Groutz nomogram, which plots free Qmax and maximum detrusor pressure (Pdet.max) measured during urodynamic studies, is one of the most popular [530] but has been suggested to overestimate obstruction [531]. The addition of fluoroscopic imaging suggested by Nitti and colleagues introduces a video-urodynamic criterion for obstruction [76]. However, both methods lack data supporting their clinical validity, especially regarding their predictive value for therapeutic intervention outcomes [74].
In a large retrospective study of 1,914 patients, 810 of whom were diagnosed with BOO, several urodynamic cut-off values were determined by ROC curve analysis to optimise the diagnostic accuracy of video-urodynamic studies [519]:
- PdetQmax > 30 cm H2O for differentiating BOO from bladder dysfunction and normal studies
(ROC AUC = 0.78); - the Abrams-Griffiths number > 30 for differentiating anatomical from functional BOO (ROC AUC = 0.66);
- PdetQmax > 30 cm H2O for differentiating dysfunctional voiding from poor relaxation of the external sphincter (ROC AUC = 0.93).
More recently, Solomon and Greenwell devised a female BOO nomogram that parallels the ICS nomogram used for male BOO [532]. It allows the calculation of an alternative BOO female index (BOOIf), using a formula closely aligned to its male counterpart: BOOIf = PdetQmax-2.2Qmax.
It is interpreted with a different algorithm however:
- BOOIf < 0: < 10% probability of obstruction;
- 5 < BOOIf < 18: equivocal, > 50% likelihood of obstruction;
- BOOIf > 18: 90% likelihood of obstruction.
The Solomon–Greenwell nomogram was the first to be tested for clinical validity. In a recent series of 21 unselected consecutive women treated for BOO, the authors observed significant improvement of all urodynamic parameters (Qmax, PdetQmax and BOOIf) in female patients who became asymptomatic postoperatively [533].
An alternative urodynamic parameter of area under the detrusor pressure curve during voiding (corrected for voided volume) has been proposed following a prospective study of 103 women [534]. The authors concluded that this variable appears to be the most discriminating urodynamic parameter for the diagnosis of female BOO. This suggested diagnostic method has not been independently validated.
Voiding cystourethrography (VCUG) alone or in conjunction with concomitant pressure–flow studies may be useful in delineating the site of obstruction. Characteristic features include:
- radiographic evidence of obstruction between the bladder neck and distal urethra in the presence of sustained detrusor contraction [76];
- lack of funnelling appearance of the bladder neck/tight bladder neck in primary bladder neck obstruction;
- proximal dilatation of the urethra with distal narrowing in women with urethral stricture disease or pelvic-floor hypertonicity.
IIt is not uncommon for women with voiding dysfunction, specifically functional BOO, to be unable to provide a flow during (video)urodynamic testing. Failure to relax the PFM can enhance the guarding reflex, limiting detrusor contractility.
4.5.4.9. Summary of evidence and recommendations for diagnosis of bladder outlet obstruction
Summary of evidence | LE |
Evaluation of LUTS by history and examination alone is insufficient to accurately diagnose female BOO. | 3 |
Urine flow studies cannot accurately diagnose BOO in women. | 3 |
Ultrasound scanning is unable to accurately diagnose BOO in women. | 2b |
Electromyography alone is unable to accurately diagnose BOO in women, although it may be of use in combination with pressure–flow studies and in differentiation of anatomical vs. functional BOO. | 3 |
Cystourethroscopy can be useful to visualise any anatomical/mechanical obstruction and provide information regarding its nature, location, and calibre. | 4 |
Urodynamics (often combined with video-fluoroscopy) is the standard test for evaluating female BOO. | 3 |
Recommendations | Strength rating |
Take a full clinical history and perform a thorough clinical examination in women with suspected bladder outlet obstruction (BOO). | Strong |
Do not rely on measurements from urine flow studies alone to diagnose female BOO. | Strong |
Perform cysto-urethroscopy in women with suspected anatomical BOO. | Strong |
Perform urodynamic evaluation in women with suspected BOO. | Strong |
4.5.5. Disease management
Therapeutic interventions for BOO aim to decrease outlet resistance in order to increase urinary flow, improve bladder emptying and thus reduce voiding and storage LUTS [74,509,529]. Treatment choice is commonly dictated by the underlying cause of the obstruction.
4.5.5.1. Conservative management
4.5.5.1.1. Behavioural modification
Behavioural modification interventions are often tailored to individual patients’ needs, symptoms and circumstances and can include elements such as education regarding normal voiding function, self-monitoring of symptoms, changes in lifestyle factors that may affect symptoms, avoidance of constipation, and alteration of voiding technique. Ultimately, techniques aim to improve the coordination between the detrusor and sphincter, resulting in their synergistic action [74,509,529].
These individual components of self-management have not been evaluated separately and most recommendations are derived from consensus methodology. They may help reduce symptoms resulting from BOO but no quantification of their effect is possible.
4.5.5.1.2. Pelvic floor muscle training +/- biofeedback
In the context of BOO, physiotherapy aims to teach patients to relax their PFMs and striated urethral sphincter during voiding. Pelvic floor muscle contraction, particularly in women with pelvic floor dysfunction, has been shown to significantly reduce vaginal resting pressure and surface EMG activity [480].
As mentioned in the section discussing UAB (Section 4.4.4.1.2), most of the evidence supporting PFMT in dysfunctional voiding is from paediatric studies.
4.5.5.1.3. Electrical stimulation
Application of electrodes that allow for controlled contraction and relaxation of the PFMs may theoretically facilitate the relaxation of the external sphincter and pelvic floor but no critical evaluation of this intervention in women with BOO has been published.
4.5.5.1.4. Use of vaginal pessary
Intravaginal devices such as pessaries aim to relieve voiding symptoms and improve bladder emptying by physical correction of the obstruction caused by a POP. In a prospective study of eighteen women with grade three or four cystocoeles and diagnosed with BOO by urodynamics (defined as PdetQmax > 25 cm H2O, Qmax < 15 mL/s), normal voiding was noted in seventeen (94%) immediately after placement of a vaginal pessary. No other outcomes were available in this series [535]. No long-term data are available on the use of vaginal pessary for BOO.
4.5.5.1.5. Urinary containment
The use of containment devices in BOO is to achieve social continence in patients with urinary retention and associated overflow UI and is often only a temporary measure. There are no published studies on the outcomes or adverse events associated with the use of urinary containment devices for the management of female BOO, though there are many involving women with UI who may have BOO as an underlying cause.
4.5.5.1.6. Urinary catheterisation
Significant urinary retention from BOO may be addressed by actively bypassing the obstruction and draining the residual urine. Catheterisation may be used as a treatment itself or as an adjunct to an initial treatment of urethral dilatation or urethrotomy or bladder neck incision. There are two ways of using a catheter: CISC or indwelling catheterisation [117].
After UI surgery, BOO may be managed by short-term catheterisation in most patients who have transient postoperative voiding difficulty. For a few women who develop chronic urinary retention, CISC or indwelling catheterisation may be offered [462].
A small RCT investigated the effectiveness of CISC to prevent recurrence after internal optical urethrotomy for urethral stricture disease. In the treatment group, CISC was done twice a day for one week, and once a day for four weeks, then once weekly for seven weeks post-urethrotomy. Freedom from stricture recurrence, determined by urethrography and uroflowmetry performed twelve weeks postoperatively, was higher in the catheterisation group compared to the group with no catheterisation (78.5% vs. 55.4%) [536]. This finding mirrors the Cochrane review on self-dilatation for urethral stricture among men that showed less recurrence with the performance of self-dilatation [537].
In a series of 20 patients with voiding dysfunction after TVT who were put on a CISC programme, overall cure rate was 59%, with cure defined as consistent residual volume < 100 mL. Half of these patients were voiding normally within twelve weeks [538].
See Section 4.4.4.1.3 for further evidence related to CISC.
4.5.5.1.7. Intraurethral inserts
An intraurethral insert is a short silicone catheter containing an internal valve and pump mechanism positioned in the female urethra. The valve-pump mechanism is operated by an external control unit, which activates to open the valve and the pump to draw urine from the bladder and allow voiding. At the end of urination, the pump ceases and the valve closes to regain continence. The insert is routinely replaced once a month.
One study reported the use of this device in 92 women with voiding dysfunction of various aetiologies including multiple sclerosis, prior pelvic surgery, pelvic radiation, diabetes mellitus, spinal stenosis and injury. The device was removed within seven days of insertion in 60% of the cases due to discomfort, peri-catheter leakage or technical difficulty. An additional 20% of patients had late discontinuation. All those who continued to use the device were satisfied, with PVR volumes remaining < 100 mL. Adverse events included migration into the bladder in six cases and symptomatic UTI in four cases [539,540]. Extended, long-term data on the use of urethral inserts are not available.
4.5.5.1.8. Extracorporeal magnetic stimulation
Extracorporeal magnetic stimulation involves the patient sitting on a device that induces consistent PFM contraction and relaxation at a set frequency and interval by repeated magnetic stimulation of motor nerve fibres. It is postulated that patients therefore learn to spontaneously contract or relax the PFM, which may enhance their ability to relax their pelvic floor while voiding [541].
In a small (n = 60) prospective non-randomised trial, alfuzosin was compared to EMS and to the combination of alfuzosin + EMS in women with functional BOO. They observed significant increase of Qmax and significant decrease of International Prostate Symptom Score (IPSS) in all groups and significantly greater improvement in the QoL question of the IPSS in the combination therapy group [541].
4.5.5.1.9. Summary of evidence and recommendations for conservative treatment of bladder outlet obstruction
Summary of evidence | LE |
Pelvic floor muscle relaxation training with biofeedback may result in relaxation of the pelvic muscles and external urethra in women with dysfunctional voiding. | 3 |
There is no available evidence in the published literature on the clinical effect of ES for management of female BOO. | NA |
In women with large (grade three or four) cystocoeles causing BOO, placement of a vaginal pessary may improve voiding efficiency. | 3 |
Regular CISC after urethrotomy is better than no catheterisation to prevent recurrence of urethral strictures. | 1b |
A CISC programme in women with voiding dysfunction after TVT has a cure rate of 59%. | 3 |
Women who use an intraurethral device have lower PVR volume, but most require its removal due to complications. | 3 |
Extracorporeal magnetic stimulation combined with alfuzosin may be more effective than either of these therapies alone in women with functional BOO. | 2a |
Recommendations | Strength rating |
Offer pelvic floor muscle training (PFMT) aimed at pelvic floor muscle relaxation to women with functional bladder outlet obstruction (BOO). | Weak |
Prioritise research that investigates and advances understanding of the mechanisms and impact of PFMT on the coordinated relaxation of the pelvic floor during voiding. | Strong |
Offer the use of a vaginal pessary to women with grade three or four cystocoeles and BOO who are not eligible/inclined towards other treatment options. | Weak |
Offer urinary containment devices to women with BOO to address urinary leakage as a result of BOO, but not as a treatment to correct the condition. | Weak |
Offer clean intermittent self-dilatation to women with urethral strictures or post-urinary incontinence surgery for BOO. | Weak |
Do not offer an intraurethral device to women with BOO. | Strong |
4.5.6. Pharmacological management
4.5.6.1. Alpha-adrenergic blockers
Alpha-adrenergic blockers are postulated to relieve LUTS caused by BOO in women via smooth muscle relaxation in the bladder neck, thus decreasing bladder outlet resistance [542].
Systematic reviews on the use of alpha-blockers in women generally involve studies with a population that includes women complaining of LUTS and voiding dysfunction. Confirmation of BOO is often not required in the trials included [543,544]. These reviews showed significant improvements in symptoms and urodynamic parameters associated with their use [543-545]. A meta-analysis of fourteen RCTs comparing alpha-blockers and placebo in women with LUTS showed significant symptom relief after alpha-blocker treatment relative to placebo, but no significant difference in Qmax, PVR volume and adverse event rates [543]. This is in contrast to prospective non-comparative trials that consistently showed improvements in voiding and storage symptoms, bother scores, and urodynamic parameters (Qmax, PVR, PdetQmax, MUCP after alpha-blocker use compared to baseline) [492,493,546-548].
A SR performed by the Panel of studies on alpha-blockers used specifically for women with BOO included one placebo-controlled RCT, one RCT comparing two types of alpha-blockers, and six prospective non-comparative studies [150]. In the only placebo-controlled RCT reporting subgroup analyses in women with urodynamically proven BOO (based on the Blaivas-Groutz nomogram) no significant difference was observed in the changes of IPSS, IPSS sub scores, Qmax, PVR volume and bladder diary after eight weeks of alfuzosin (n = 58) vs. placebo (n = 59). Of note, no EMG and/or voiding cysto-urethrography was used to distinguish between dysfunctional voiding and primary bladder neck obstruction [549].
Information on the comparative effectiveness of the different types of alpha-blockers was limited to one RCT. A small trial of 37 women with IPSS > 8, Qmax < 12 mL/s and PVR volume > 50 mL, compared tamsulosin and prazosin over a three-month treatment period. More patients treated with tamsulosin were completely satisfied with their treatment (16/20 vs. 9/20). Both treatment groups showed significant improvement in symptom scores from baseline but no further statistical comparison between the groups was done. However, a larger decrease in AUA symptom score was seen in the tamsulosin group compared with the prazosin group. More adverse events were reported with prazosin (thirteen vs. one case) [550].
4.5.6.2. Striated muscle relaxants
Baclofen is a gamma-aminobutyric acid (GABA) agonist that exerts its effect on the GABAergic interneurons in the sacral inter-mediolateral cell column responsible for the relaxation of the striated urinary sphincter during voiding.
A randomised placebo-controlled crossover trial investigated the efficacy and safety of a four-week course of oral baclofen 10 mg three times/day in 60 women diagnosed with BOO, based on increased EMG activity with sustained detrusor contraction during voiding. It showed a lower number of voids, significant improvements in Qmax and PdetQmax with baclofen compared with placebo. PVR volume, maximum cystometric capacity and MUCP were not significantly different between the groups. Adverse event rates were also similar, with the most common being somnolence, dizziness, and nausea. An important limitation of this study was the lack of patient-reported outcomes to assess symptoms and QoL [551].
4.5.6.3. Oestrogens
The relative reduction in urethral wall compliance seen in atrophic urethritis due to oestrogen deprivation may be responsible for urethral obstruction in postmenopausal women. Oestrogen therapy is thus theoretically expected to improve the condition. There are no published studies on the use of oestrogens specifically for the management of female BOO.
4.5.6.4. Sildenafil
Sildenafil, by inhibiting phosphodiesterase five, increases the levels of nitric oxide in the female urethral sphincter, thereby promoting urethral relaxation.
A placebo-controlled, randomised crossover trial that included twenty women with partial or complete retention or obstructive voiding, with high MUCP and elevated US-estimated sphincter volume (> 1.6 cm) showed that while there was significant improvement in symptom scores and urodynamic parameters from baseline with sildenafil treatment, this difference was not significant when compared with placebo [552].
4.5.6.5. Thyrotropin-releasing hormone
Intravenous thyrotropin-releasing hormone (TRH) has been postulated as a neurotransmitter that induces urethral relaxation [553]. The exact mechanism is unclear.
In a small RCT of sixteen women with voiding difficulty, eight (three with BOO) were randomised to receive 200 μg intravenous bolus of TRH, and eight (three with BOO) received saline. No difference in the decline in functional profile lengths and maximum urethral closure pressures were noted between treatment groups, despite a significant decline noted from baseline in the treatment group. No subgroup analysis of women with BOO was reported [553].
4.5.6.6. Summary of evidence and recommendations for pharmacological management
Summary of evidence | LE |
Alpha-adrenergic blockers may be associated with improvement in symptom scores from baseline, but not urodynamic parameters compared with placebo. | 1a |
Tamsulosin is associated with greater improvement in symptom score compared with prazosin. | 1b |
Oral baclofen is better than placebo in improving Qmax and PdetQmax, but not other urodynamic parameters. Its effects on symptoms are not well reported. | 1b |
Current evidence does not show that sildenafil is superior to placebo in improving symptoms or urodynamic parameters of female patients with BOO. | 1b |
Trials including women with voiding problems of mixed aetiologies showed no difference in urodynamic outcomes between intravenous TRH and placebo. | 1b |
Recommendations | Strength rating |
Offer uroselective alpha-blockers, as an off-label option, to women with functional bladder outlet obstruction (BOO) following discussion of the potential benefits and adverse events. | Weak |
Offer oral baclofen to women with BOO, particularly those with increased electromyography activity and sustained detrusor contraction during voiding. | Weak |
Only offer sildenafil to women with BOO as part of a well-regulated clinical trial. | Strong |
Do not offer thyrotropin-releasing hormone to women with BOO. | Strong |
4.5.7. Surgical management
4.5.7.1. Intra-sphincteric botulinum toxin injection
Botulinum toxin inhibits the presynaptic release of acetylcholine, which reduces urethral sphincter tone. It is also believed to decrease the release of noradrenaline in the urethra to counteract external urethral sphincter overactivity [554].
Evidence on the use of botulinum toxin for female BOO is limited to small case series. Most studies included mixed populations without subgroup analyses, or the diagnosis of voiding dysfunction could not be ascertained as solely resulting from BOO. No comparative trial exclusively involving female BOO patients using botulinum toxin has been identified in the literature.
A SR including several reports of small case series using variable doses of onabotulinumtoxinA injected periurethrally in women with dysfunctional voiding showed improvements in symptoms, and reductions in residual volume and voiding detrusor pressure. Larger series in adults (both sexes) showed success rates of 86–100% [554].
A double-blind, placebo-controlled RCT (n = 73) resulted in significantly lower IPSS score and larger voided volume after 100 U onabotulinumtoxinA compared with saline in 31 men and women with dysfunctional voiding. Dysfunctional voiding was defined by a spinning top appearance on real-time fluoroscopy, poorly relaxed urethral sphincter on EMG, and a normal-to-high voiding pressure with a low and/or intermittent urinary flow rate, a PVR volume > 300 mL, and a low voiding efficiency. Other urodynamic parameters were comparable between the groups [555]. A subgroup analysis on the female population of this study was not available.
Two small case series in women with BOO reported the effects of intrasphincter 100 U onabotulinumtoxinA. Both showed improvement in symptom and bother scores and significant reduction in PVR volume [513,556]. One study reported increased Qmax and improved static urethral pressure profile (UPP) [513]. The average symptom-free duration was 16.8 weeks in another study [556]. Adverse events included UTI and temporary need for CISC. No SUI was reported.
4.5.7.2. Sacral nerve stimulation
Sacral nerve stimulation is postulated to decrease urethral tone and to work by blockade of the inhibitory urethral afferent impulses, which cause inhibition of normal bladder contraction.
No comparative trial has been identified in the literature on the use of neuromodulation for female BOO.
Most publications on neuromodulation for voiding dysfunction are retrospective reviews of cases, involving a mix of patient populations who underwent the procedure for different indications. In studies that indicated a subgroup of patients with urinary retention, there was either no urodynamic confirmation of the nature of the retention or separate outcomes were not reported for participants with retention.
A review of 60 women who underwent SNS for urinary retention associated with outlet obstruction (defined as UPP > 100 cm H2O, increased urethral sphincter volume > 1.8 mL, and abnormal EMG with repetitive discharges and decelerating bursts) showed an overall spontaneous voiding rate of 72% over a mean follow-up of four years. Of those who continued to require CISC up to twice daily postoperatively, the frequency was less than prior to surgery (degree not specified). There were 99 adverse events and 63 surgical revisions. In this series, half of the patients underwent a one-stage SNS procedure and the other half a two-stage procedure. The proportion of patients who required CISC-assisted voiding was higher in the two-stage group (27% vs. 17%). More serious adverse events (defined as events requiring admission or surgical revision to resolve issues such as loss of response, lead migration and surgical revisions) were associated with the one-stage procedure [557].
4.5.7.3. Pelvic organ prolapse surgery
Pelvic organ prolapse surgery may relieve BOO by correcting the urethral kinking caused by the prolapse or by relieving the urethral compression brought about by the prolapsing organ [74,509,529].
Bladder outlet obstruction due to POP may be addressed by corrective surgery. Based on reviews, the majority of patients who had BOO caused by POP who had repair of their cystocoele demonstrated improvement of their voiding difficulties [462,558].
A multicentre prospective study involving 277 women with at least grade two symptomatic POP who underwent surgery demonstrated a significant reduction in voiding symptoms and PVR volume one year postoperatively [559].
A retrospective study of 50 women who underwent laparoscopic sacrocolpopexy for POP showed a significant increase in mean postoperative Qmax and decrease in PdetQmax and PVR in those aged > 65 years. The OAB symptom score improved but there was no significant difference in the ICIQ-SF score postoperatively [560].
4.5.7.4. Urethral dilatation
Urethral dilation involves the passage of sequentially greater diameter dilators into the urethra, causing the obstructing fibrotic tissue to break open, thereby widening the lumen. It is considered the primary procedure of choice for women suspected of urethral stricture disease [527]. Dilation of up to 30–40 Fr has been done. There is no standard dilatation technique; dilatation of up to 43 Fr has been described, although other authors suggest dilating to 30 or 35 Fr.
A systematic review of female urethral stricture management included three trials involving urethral dilatation. Pooled analysis of data from 93 women showed a mean success rate of 49% after urethral dilation to 41 Fr with a mean follow-up of 46 months. Mean time to failure was 12 months. In treatment-naïve patients, success rate (as defined by trialists) was 58%, compared with 27.2% in patients who had undergone previous dilatation [561].
An RCT of 50 women with OAB syndrome and associated urodynamically confirmed BOO (defined as a
Qmax < 15 mL/s with a voided volume of > 100 mL and/or PVR volume > 200 mL, not due to urethral stricture) compared the effect of cystoscopy and bladder distension with urethral dilatation (n = 22) and cystoscopy only (n = 28) after six weeks’ follow-up. Significantly more patients who had cystoscopy only had persistent urgency at six weeks and six months postoperatively. Urodynamic parameters did not significantly change pre- and postoperatively in both groups. The greater improvement in QoL scores based on the King’s Health Questionnaire domain scores seen in the non-urethral dilatation group in this trial should be interpreted cautiously because of the higher baseline scores. There were no significant changes in Qmax, PVR volume, voided volume or PdetQmax in any of the two groups at six weeks’ questioning the role of any of these two options for therapeutic management of BOO. Also, six patients (12%) developed postoperative SUI [562].
A prospective trial of 86 women with primary urethral stricture compared on-demand vs. intermittent urethral dilatation to 24 Fr every two months. It showed an overall increase in Qmax and decrease in PVR volume post-dilatation. Significantly greater improvements were seen in the intermittent urethral dilatation group [563].
Worsening or new-onset SUI is a concern with urethral dilatation, but it is less of a concern than after urethrotomy or surgical reconstruction. Patients have also reported frequency and urgency post-dilatation [564].
4.5.7.5. Urethrotomy
Urethrotomy involves incision of the urethra endoscopically or using a urethrotome. It addresses the urethral narrowing by cutting open the scar tissue which is causing the obstruction [74,509,529,564].
A prospective study of ten women with urethral strictures investigated the effect of Otis urethrotomy to 40 Fr followed by six weekly dilatations. There was significant improvement in IPSS, QoL, voided volume, Qmax and PVR volume at six months. Only the improvements in PVR volume and QoL were maintained on long-term follow-up (mean 82 months) [565].
4.5.7.6. Bladder neck incision/resection
Transurethral bladder neck incision decreases resistance at the bladder neck by cutting open the hypertrophic bladder neck smooth muscle in patients with primary bladder neck obstruction. Transurethral incision of the bladder neck may be performed with a unilateral incision at the twelve o’clock position or with bilateral incisions at the five and seven o'clock, two and ten o'clock or three and nine o’clock positions, or four incisions at the three, six, nine and twelve o’clock positions. This may be done using a resectoscope with a Collin’s knife, cold knife, or using laser energy. Some authors report additional resection of the bladder neck between the five and seven o’clock positions.
A review of non-comparative studies on bladder neck incision for the treatment of bladder neck obstruction in women reports success rates of 76–100% [512].
Bladder neck incision was compared with V-Y-reconstruction using Nesbit’s technique in a retrospective study of seventeen women with BOO, diagnosed by various uroradiological, endoscopic and urodynamic investigations. The results showed similar symptomatic improvement rates and postoperative PVR volume between the two groups. V-Y plasty had a longer operating and catheter time, lower uroradiological improvement rate, higher transfusion rate, and higher adverse event rate [566].
Several prospective case series consistently reported significant improvements in IPSS, QoL, Qmax, PdetQmax and PVR volume after treatment compared to baseline, regardless of the site of the incision, type of energy used or the length of follow-up [567-570].
The largest case series with 84 patients diagnosed with primary bladder neck obstruction (based on lack of funnel shape of the bladder neck during voiding-on-voiding cysto-urethrography, Pdet > 20 cm H2O and Qmax < 12 mL/s) showed success in 84.5% of patients with improvement in IPSS, QoL, Qmax and PdetQmax after mean follow-up of 27.4 months (6–78 months). Complications included vesico-vaginal fistula (VVF) (3.6%), SUI (4.7%) and urethral stricture (3.6%) [567].
No comparisons have been made between the different incision techniques (location, length, and depth of incision, implement used – cold knife vs. hot knife vs. laser, with or without resection). However, in a case series of 84 patients, complications of VVF and SUI were noted in the cohort of patients who had their incisions at five and
seven o’clock positions, and not in those who had their incisions at two and ten o’clock [567].
Adverse events include SUI, requirement for reoperation, and recurrence. Postoperative SUI was reported in 3– 33% [512].
4.5.7.7. Urethroplasty/urethral reconstruction
Surgical reconstruction of the female urethra has been used in the management of extensive urethral stricture. Several urethroplasty techniques include the use of vaginal or labial flaps, as well as vaginal and buccal grafts after cutting open the fibrotic tissue causing the urethral obstruction [571]. The use of bladder flaps has also been reported [572], and laboratory-engineered tissue grafts have also been used [572].
The surgical approaches have been described based on the position relative to the urethra; dorsal, ventral, or circumferential. The dorsal approach is believed to provide better mechanical support and a more vascularised bed for a graft or flap. However, there is greater risk of damage to the sphincter and clitoral bodies with this approach. The ventral approach is more familiar to most surgeons and requires less urethral mobilisation. However, it is reported as being more prone to urethrovaginal fistulae, although it is not clear to what extent [527].
Reviews of studies reporting outcomes of urethroplasty state success rates of 57–100% [573]. Pooled analysis from six studies using vaginal or labial flaps showed a mean success rate of 91% with a mean follow-up of 32 months. Vaginal or labial graft urethroplasty was reported to have an 80% success rate with a mean follow-up of 22 months.
Oral mucosal grafts, reported in seven studies, had a mean success of 94% after a mean follow-up of fifteen months [527]. A later review of studies on dorsal buccal mucosal graft reported success rates of 62–100%, with a pooled success rate of 86% [574]. A long-term study with a mean follow-up of 32 months showed a stricture recurrence rate of 23.1% [573].
4.5.7.8. Urethrolysis
Bladder outlet obstruction in women occurring as a complication of surgery for SUI may be managed surgically by urethrolysis, to regain urethral mobility. Urethrolysis may involve removal of peri-urethral anti-incontinence sutures, scar tissue and fibrosis.
Case series showed success rates measured as improved voiding and lower residual volumes, improvement, or resolution of symptoms and QoL, and improvement of urodynamic parameters after treatment [575-577]. De novo SUI was reported in 39% in one study [577]. Another study reported an association of persistent postoperative bladder symptoms with greater delay to performing urethrolysis [578].
4.5.7.9. Removal/excision/section/loosening of mid-urethral sling
In women who develop BOO after placement of a mid-urethral sling, surgical management may include tape loosening, incision or division, and excision and/or removal of the tape [462].
Several small retrospective reviews of cases using different techniques of sling revision (incision, partial excision, or excision) showed good success rates in terms of symptom reduction, resumption of voiding with significant reduction in PVR volume and improvement of urodynamic parameters. Stress urinary incontinence recurs in a small proportion of patients and often to a lesser degree than prior to the sling procedure. Studies have shown long-term efficacy, including preservation of continence.
In a series of 63 women who presented with voiding dysfunction and persistent PVR volume > 100 mL after tape surgery for UI, different techniques were compared. Comparisons involved sling revision: sling division (n = 46) vs. partial sling excision (n = 13) vs. sling revision (division or excision) with an additional anti-SUI procedure (n = 4). The authors reported an overall success rate of 87% (PVR volume < 150 mL). No significant difference in success rates was demonstrated among the different revision techniques. There was a greater need for surgery for recurrent SUI in the partial sling excision group without an anti-SUI procedure (23% vs.
2.2 and 0) [579].
One study showed that patients who underwent surgical release > 180 days after initial anti-UI surgery had significantly less recurrent SUI compared with patients who underwent the release sooner (15% vs. 46%) [580].
4.5.7.10. Summary of evidence and recommendations for surgical management of bladder outlet obstruction
Summary of evidence | LE |
Intrasphincteric injection of botulinum toxin results in the improvement of symptoms and urodynamic parameters. | 2 |
Sacral nerve stimulation results in spontaneous voiding and a reduction in CISC rate in the majority of female BOO patients in idiopathic urinary retention. | 3 |
More serious adverse events and surgical revisions were associated with the one-stage neuromodulator implantation procedure. | 3 |
Repair of POP improved PVR and voiding symptoms. | 3 |
Urethral dilatation in women with BOO results in significant improvement in OAB symptoms, but improvements in urodynamic parameters of voiding are inconsistent. | 1b |
Programmed intermittent urethral dilatation results in better outcomes compared with on-demand dilatation. | 3 |
Effects of urethral dilation are poorly sustained, requiring repeat intervention in the long term. | 3 |
Internal urethrotomy followed by regular dilatations resulted in significant improvement in symptoms and urodynamic parameters in women with BOO. | 3 |
Bladder neck incision in females with BOO results in improvements in symptoms and urodynamic parameters. | 3 |
Complications of bladder neck incision are not common, but include VVF, SUI, and urethral stricture. | 3 |
Urethroplasty using grafts or flaps in women with BOO due to urethral stricture have good success rates with significant improvements of symptoms, QoL scores and urodynamic parameters compared to baseline. | 3 |
Urethroplasty results in better QoL and Qmax compared to urethral dilatation. | 2 |
Long-term results showed significant stricture recurrence rate after urethroplasty. | 3 |
Urethrolysis performed on women with voiding problems after anti-UI surgery resulted in improvements in symptoms, QoL and urodynamic parameters post-operatively. | 3 |
Delayed urethrolysis was associated with persistent post-operative bladder symptoms. | 3 |
Sling revision in women who presented with urinary retention or voiding problems and significant PVRs after sling surgery for UI resulted in improvements in symptoms and urodynamic parameters, resumption of voiding and reductions in PVRs. | 3 |
Sling revision is associated with the risk of recurrent SUI. | 3 |
Recommendations | Strength rating |
Offer intra-sphincteric injection of botulinum toxin to women with functional bladder outlet obstruction (BOO). | Weak |
Offer sacral neuromodulation to women with functional BOO. | Weak |
Advise women with voiding symptoms associated with pelvic organ prolapse that symptoms may improve after surgery. | Weak |
Offer urethral dilatation to women with urethral stenosis causing BOO but advise on the likely need for repeated intervention. | Weak |
Offer internal urethrotomy with postoperative urethral self-dilatation to women with BOO due to urethral stricture disease but advise on its limited long-term improvement and the risk of postoperative urinary incontinence (UI). | Weak |
Do not offer urethral dilatation or urethrotomy as a treatment for BOO to women who have previously undergone mid-urethral synthetic tape insertion due to the theoretical risk of causing urethral mesh extrusion. | Weak |
Inform women of limited long-term improvement (only in terms of post-void residual volume and quality of life) after internal urethrotomy. | Weak |
Offer bladder neck incision to women with BOO secondary to primary bladder neck obstruction. | Weak |
Advise women who undergo bladder neck incision on the small risk of developing stress urinary incontinence (SUI), vesico-vaginal fistula or urethral stricture postoperatively. | Strong |
Offer urethroplasty to women with BOO due to recurrent urethral stricture after failed primary treatment. | Weak |
Caution women on the possible recurrence of strictures on long-term follow-up after urethroplasty. | Weak |
Offer urethrolysis to women who have voiding difficulties after anti-UI surgery. | Weak |
Offer sling revision (release, incision, partial excision, or excision) to women who develop urinary retention or significant voiding difficulty after tape surgery for UI. | Strong |
Caution women about the risk for recurrent SUI and the need for a repeat/concurrent anti-UI surgery after sling revision. | Strong |
4.5.8. Follow-up
Women with BOO should be followed up and monitored regularly due to the risk of further deterioration of voiding or renal function in case of persistence and progression of the obstruction. For those who received treatment, monitoring must be done for recurrence of BOO. In particular, women who undergo urethral dilation, urethrotomy or urethroplasty for urethral stricture need to be monitored for stricture recurrence.
4.6. Nocturia
Nocturia was defined by the ICS in 2002 as “the complaint that the individual has to wake at night one or more times to void” and quantified in an updated document in 2019 as “the number of times an individual passes urine during their main sleep period, from the time they have fallen asleep up to the intention to rise from that period” [581]. The EAU Guidelines Panel on Urinary Incontinence conducted a SR on nocturia in women [582]. The search covered evidence up to 2017 and this review was updated with a scoping search in 2020.
4.6.1. Epidemiology, aetiology, pathophysiology
The prevalence of nocturia varies according to age with 4–18% of women aged 20–40 years experiencing > 2
episodes per night, compared to 28–62% of women aged > 70 years [583]. In a study of 1,000 community-dwelling older adults, female nocturia was associated with older age, African American race, history of UI, lower limb oedema and hypertension [584]. A report on > 5,000 adults aged 30–79 years identified around 28% with nocturia and found additional correlates with increased cardiac disease, type 2 diabetes, and diuretic use [585]. A SR and meta-analysis with moderate certainty evidence based on the GRADE approach, demonstrated that the higher incidence of nocturia among hypertensive patients was more strongly associated (1.2 to 1.3-fold) among Black and Asian women, unrelated to their age or BMI status [586]. Another SR with moderate certainty of evidence based on the GRADE approach showed that nocturia was associated with a 1.2-fold increased risk of falls and possibly an approximately 1.3-fold increased risk of fractures [587]. Another SR and meta-analysis concluded that nocturia is probably associated with an ~1.3-fold increased risk of death [587].
The aetiology of nocturia is multifactorial and can include both urological and non-urological causes. Urological conditions which may exhibit nocturia as a significant symptom include OAB syndrome, BOO, DU, and dysfunctional voiding. Non-urological causes include 24-hour polyuria (which includes nocturnal polyuria), congestive heart failure, sleep apnoea, restless leg syndrome, peripheral vascular disease, sleep disorders, night-time food ingestion, dependent oedema, and excessive fluid intake [588]. Given the varied aetiology of this symptom, there are a range of possible pathophysiological mechanisms, including: (1) 24-hour polyuria (e.g., diabetes mellitus, primary polydipsia, and diabetes insipidus); (2) nocturnal polyuria (e.g., behavioural, peripheral oedema, obstructive sleep apnoea, glycosuria, hormonal abnormalities and cardiac dysfunction ); (3) diminished bladder capacity (e.g., OAB syndrome/DO, PFM dysfunction, BOO, pharmaceuticals, LUT calculi or tumours, and neurological bladder dysfunction); and (4) primary or secondary sleep disorders [589].
In postmenopausal women the relative deficiency in endogenous oestrogen production is thought to exacerbate all major pathophysiological mechanisms that may underlie nocturia [590].
4.6.2. Classification
Classification of nocturia is dependent on bladder diary analysis and several parameters have been defined as important [591]:
- nocturnal urine volume – total volume of urine passed during the night (this includes the first morning void but does not include the last void prior to sleep);
- maximum voided volume – largest single voided volume in 24 hours;
- nocturia index – nocturnal urine volume divided by maximum voided volume;
- nocturnal polyuria index – nocturnal urine volume divided by 24-hour urine volume;
- nocturnal urine production – nocturnal urine volume divided by duration of sleep, in hours.
Analysis of these parameters allows clinical classification of nocturia based on physiological abnormalities that can cause nocturia:
- 24-hour polyuria;
- nocturnal polyuria;
- diminished bladder capacity;
- sleep disorders.
4.6.3. Diagnostic evaluation
Evaluation of nocturia should include a thorough medical history and physical examination with particular reference to history of sleep disorders, fluid balance, associated LUTS, cardiovascular and endocrine co-morbidity, renal disease, current medications, and history of urological disease [591,592]. There are several nocturia-specific symptom scores, such as the ICI Questionnaire-Nocturia, Nocturia Quality of Life Questionnaire (N-QoL), and Nocturia Impact Diary; some of which were developed in men. These questionnaires have shown good content and discriminant validity, reliability, and sensitivity to change as well. A further screening tool that aims to identify causes of nocturia is the Targeting the individual’s Aetiology of Nocturia to Guide Outcomes (TANGO) assessment tool [593-595]. The PLANET study (PLanning Appropriate Nocturia Evaluation and Treatment) has suggested a useful tool for initial history taking called the SCREeN tool, with questions focused on evaluating areas of Sleep, Cardiovascular, Renal, Endocrine and Neurological function [596].
A bladder diary is a vital initial investigation tool in patients complaining of nocturia and further supplementary investigations are guided by any abnormalities identified. Bladder diary analysis can allow for calculation of the parameters detailed in Section 4.6.2. A low nocturnal bladder capacity or global bladder capacity will be highlighted by reduced voided volumes during nocturnal hours or both night and day. This suggests an underlying urological condition such as OAB syndrome, BOO or DU. The term 24-hour polyuria is defined as 24-hour urine production > 40 mL/kg [597] and may be present in conditions such as diabetes mellitus or diabetes insipidus. The definition of nocturnal polyuria is age dependent and the thresholds for this diagnosis range from 20% (in younger persons) to 33% (age > 65 years) of the 24-hour urine volume produced during sleep. This may also be observed in patients with loss of circadian rhythm, cardiovascular disease, sleep apnoea, or sleep disorders [591]. A large study conducted across European and American centres involving ~2,000 patients identified nocturnal polyuria as a contributory cause of nocturia in 89% of patients who were being treated for LUT abnormalities such as OAB syndrome or benign prostatic enlargement [598].
As an alternative to the > 3-day bladder diary a nocturnal-only diary has been investigated in men [599]. The results showed acceptable sensitivity and specificity for the nocturnal bladder diary compared with the standard bladder diary for most parameters. The nocturnal-only diary was not able to diagnose 24-hour polyuria and has not yet been validated for use in women.
A 2022 SR and nominal group technique (NGT) consensus exercise based on fourteen observational studies of mixed populations recommended including blood tests for renal function, thyroid function, HbA1c and calcium levels in the initial work-up of patients presenting with nocturia [600-602].
Sleep disorders are potentially highly influential in nocturia, but often overlooked. A 2022 SR and NGT expert consensus based on thirteen mixed studies (nine cohort, three cross-sectional and one case-control) recommended the use of screening questions to reach a clinical diagnosis of sleep disorder (insomnia, restless legs syndrome/periodic limb movements of sleep and parasomnias) to offer conservative treatment within primary care [601].
4.6.3.1. Summary of evidence and recommendations for diagnosis of nocturia
Summary of evidence | LE |
A thorough medical history is an integral part of the evaluation of women presenting with nocturia, including screening for sleep disorders. | 4 |
Nocturia-specific questionnaires are sensitive to symptom changes. | 3 |
A bladder diary allows for calculation of important indices and can identify potential causes of nocturia. | 3 |
Nocturnal-only bladder diaries have been evaluated in men only. | 3 |
Consider renal function, thyroid function, HbA1c and calcium level blood tests in the initial workup of women presenting with nocturia. | 2 |
Recommendations | Strength rating |
Take a complete medical history from women with nocturia, including screening for sleep disorders. | Strong |
Use a validated questionnaire during assessment of women with nocturia and for re-evaluation during and/or after treatment. | Weak |
Use a three-day bladder diary to assess nocturia in women. | Strong |
Do not use nocturnal-only bladder diaries to evaluate nocturia in women. | Weak |
Consider screening for sleep disorders and performing renal function, thyroid function, HbA1c and calcium level blood tests in the initial workup of women presenting with nocturia as predominant symptom. | Strong |
4.6.4. Disease management
When evaluating the results of trials involving treatment strategies for nocturia, it is vital to examine for clinical significance as statistical significance can be achieved with small reductions in nocturia episodes.
4.6.4.1. Conservative management
The individual components of self-management have not been critically evaluated and most recommendations are traditionally derived from consensus methodology. Interventions such as those listed below may help with nocturia but, for the majority, no quantification of their effect is possible:
- reduction of fluid intake at specific times;
- avoidance/moderation of intake of caffeine or alcohol;
- distraction techniques;
- bladder retraining;
- pelvic floor muscle training;
- reviewing medication;
- treatment of constipation.
The available data for conservative treatment of nocturia show significant heterogeneity. In a SR [582], three studies [603-605] were favourable for conservative treatment with PFMT, with another failing to confirm a benefit [606].
The highest level of evidence comes from a study of 131 patients (a secondary analysis from a prospective RCT that had urgency-predominant UI as the primary inclusion criterion). The study found that training in PFM contraction, which included four sessions of biofeedback-assisted PFMT, reduced nocturia by a median 0.50 episodes per night and was significantly more effective than anticholinergic drug treatment or placebo [603]. The certainty of evidence associated with this treatment is moderate.
A smaller RCT of 50 women with urinary complaints, randomised 1:1 to BT and PFMT compared with a control group receiving no treatment, showed a significant decrease in patients’ complaints of nocturia [604]. Another RCT in only 24 women compared PFMT only to Interferential Therapy plus [605]. Although the authors did not find significant differences between the groups, the change in nocturia episodes before and after treatment was statistically significant in both groups. This study was underpowered by the authors’ own admission. The level of certainty of the evidence from these two trials is low. A large randomised, two-arm, parallel design, superiority trial (n = 647; women), compared the effects of unsupervised behavioural PFMT programmes delivered in a two-hour class format and 20 minutes video format on UI prevention. No significant between-group differences of nocturia were observed at 3 months and 12 months, but at 24 months, women in the 2 hour class group were less likely to have fewer nocturia episodes (OR = 0.5; 95 % CI: 0.3−0.7; p = 0.005) compared with those in the 20 minutes video group, but the authors concluded that the evidence is not sufficient to support one management strategy [605].
A multicentre, open-labelled, RCT evaluated whether cognitive behavioural therapy (CBT) using a self-assessment via a checklist is effective in improving nocturia in a mixed population (30/78 women). The mean rate of achievement of the CBT group was 64.4%. There was no significant difference between the two groups in night-time frequency based on the IPSS Q7 at four weeks but episodes of nocturia on the frequency volume chart (FVC) were significantly smaller in the CBT group (1.9 ± 0.9) than in the control group (2.4 ± 1.3; p = 0.039) [607].
In a secondary analysis from a prospective RCT, 210 women with urgency UI (UUI) were evaluated for change from baseline in the number of episodes of nocturia and nocturnal incontinence between groups allocated to medical treatment (tolterodine ER 4 mg) alone vs. medical treatment plus PFMT [606]. No significant difference between the groups was found and the actual difference in nocturia episodes in either treatment arm was small. The level of certainty of the evidence from this trial is low.
A recent RCT has explored both individual and group PFMT with a specific secondary outcome of number of patients with two or more nocturia episodes per night [319]. The authors reported similar reductions, with > 30% of patients who had > 2 episodes of nocturia at baseline no longer experiencing this level of symptoms at one year after PFMT.
One small, single-centre RCT in which functional magnetic stimulation was compared with no treatment in 39 women reported a significant decrease in nocturia (together with voiding frequency and pad use) in the treatment group compared with the control group [608].
In patients with obstructive sleep apnoea who complain of nocturia, continuous positive airway pressure has been shown to be effective in a SR and meta-analysis of five RCTs involving both sexes [609]. This treatment was associated with an average numerical reduction in nocturia of > 2 episodes per night.
4.6.4.1.1. Summary of evidence and recommendations for conservative management of nocturia
Summary of evidence | LE |
Individual or group PFMT appears to be equally effective for reduction in nocturia episodes. | 1b |
Most studies evaluating PFMT for nocturia in women with additional urinary symptoms have shown positive results compared with placebo or anticholinergic drugs. | 1b |
Treatment of nocturia secondary to obstructive sleep apnoea with continuous positive airway pressure reduces nocturia episodes. | 1a |
Recommendations | Strength rating |
Offer women with lower urinary tract symptoms (LUTS) lifestyle advice prior to, or concurrent with, treatment. | Strong |
Offer pelvic floor muscle training for nocturia (either individually or in the group setting) to women with urinary incontinence or other storage LUTS. | Strong |
Offer women with nocturia and a history suggestive of obstructive sleep apnoea a referral to a sleep clinic for assessment of suitability for continuous positive airway pressure treatment. | Strong |
4.6.4.2. Pharmacological management
4.6.4.2.1. Desmopressin
Desmopressin is a synthetic analogue of the hormone vasopressin and is most often used for management of nocturia due to nocturnal polyuria. In a SR [582], three trials specifically conducted in women were found but more additional data could be extracted from studies in mixed populations. The earliest evidence comes from a 1982 single-site crossover trial involving 25 women treated with 20 g desmopressin or placebo and revealed a significant decrease in nocturnal urine output at six weeks [610]. A more recent multicentre, multinational double-blind RCT involving 141 women used desmopressin 0.1, 0.2 or 0.4 mg orally at bedtime after a dose-titration period [611]. This increased the likelihood of a positive outcome because non-responders were excluded at that stage. At three weeks, significant reductions in nocturnal urinary frequency and nocturnal diuresis were reported. In another multicentre double-blind RCT, 58 women were randomised into five groups (twelve receiving placebo, twelve desmopressin 10 μg, eleven desmopressin 25 μg, eleven desmopressin 50 μg and twelve desmopressin 100 μg) for four weeks [612]. A dose–response relationship was observed, and women appeared more sensitive than men to desmopressin. Significant changes in nocturnal urine volumes were reported in favour of the higher desmopressin doses. Differences in the nocturnal polyuria index also tended to favour desmopressin over placebo and the higher desmopressin doses. The level of certainty of the evidence from these trials is low.
Desmopressin can be safely combined with anticholinergics with significant benefit in women with OAB and nocturnal polyuria, as shown by a multicentre RCT of 97 patients [613]. A post hoc analysis of data comparing three-month once-daily combination (desmopressin 25 μg/tolterodine 4 mg, n = 49) or monotherapy (tolterodine 4 mg/placebo, n = 57) revealed a significant reduction in nocturnal void volume and time to first nocturnal void in favour of combination therapy. The level of certainty of the evidence from this trial is moderate.
Pooled data from three RCTs were used to examine the adverse event profile of desmopressin, specifically hyponatraemia [614]. The authors reported that the majority tolerate desmopressin treatment without clinically significant hyponatraemia, but risk increased with age and lower baseline serum sodium concentration. They advised that desmopressin treatment in elderly patients should include careful monitoring of the serum sodium concentration and should be avoided in patients with a baseline serum sodium concentration below normal range.
4.6.4.2.2. Anticholinergics
A SR [582] identified three RCTs involving anticholinergics such as oxybutynin 2.5 mg/day [603] and tolterodine 4 mg/day [606,613]. A secondary analysis from a prospective RCT involving 131 women with nocturia followed up for eight weeks found that women receiving 2.5 mg immediate-release oxybutynin once daily (with the possibility of self-titration and dose escalation to 5 mg three times daily) had fewer nocturia episodes than women receiving placebo [603]. Women receiving oxybutynin plus behavioural therapy also exhibited a significant decrease in nocturia episodes compared with placebo and oxybutynin alone. A multicentre RCT with 305 women followed up for eight weeks examined the efficacy of tolterodine tartrate 4 mg alone or in combination with behavioural training [606]. Significant differences compared with baseline were observed in mean nocturia episodes and nocturnal incontinence episodes in both groups, but no difference was reported between the two treatment groups. The level of certainty of the evidence from this trial is moderate.
In an RCT including 97 women with nocturnal polyuria and OAB syndrome, comparing three months of once daily combination (desmopressin 25 μg/tolterodine 4 mg, n = 49) or monotherapy (tolterodine 4 mg/placebo, n = 57), a significant reduction in mean number of nocturnal voids compared with baseline was reported in both groups [613]. The level of certainty of the evidence from this trial is moderate.
A large comparative study followed 407 women with OAB and nocturia for four weeks [615]. The patients were given tolterodine as monotherapy in one group, and tolterodine combined with estazolam (a benzodiazepine) in the other group. Significant changes from baseline in both groups for the main outcome of number of nocturia episodes were reported. Combination therapy showed a significant benefit for women with OAB and nocturia compared with monotherapy in terms of differences in number of nocturia episodes, urgency episodes in 24 hours, UUI episodes in 24 hours, and voided volume per micturition. The level of certainty of the evidence from this trial is very low.
A small multicentre RCT compared oxybutynin patch vs. mirabegron on nocturia-related QoL in women with OAB. Both treatments showed improvements in N-QoL score at four weeks, but mirabegron showed statistical differences at eight weeks. Additionally, only mirabegron decreased nocturnal frequency and water intake, and prolonged hours of uninterrupted sleep eight weeks after administration with statistical significance, whereas oxybutynin patch did not [616].
4.6.4.2.3. Oestrogens
In a SR [582], only a single RCT investigating the efficacy of oestrogen for nocturia was identified [617]. This trial compared an oestradiol-releasing vaginal ring with an oestriol vaginal pessary in 251 women followed up for six months. There was no difference between the treatment groups in the number of women reporting nocturia, although they reported significant change from baseline in both treatment arms with > 50% of subjects responding in each arm. The certainty of evidence for this outcome was low.
4.6.4.2.4. Diuretic treatment
In a randomised placebo-controlled study an afternoon dose of 40 mg furosemide (taken six hours before bedtime) in an attempt to establish complete diuresis before bedtime was given to elderly men [618]. In the 43 men who completed the study, night-time frequency in the furosemide group fell by 0.5 episodes compared with placebo, and percentage night-time voided volume fell by 18%. No such study has been carried out in female patients.
4.6.4.3. Summary of evidence and recommendations for pharmacological management of nocturia
Summary of evidence | LE |
Desmopressin treatment for nocturia shows significant reductions in nocturnal urine output, nocturnal urinary frequency, and nocturnal polyuria index. | 1b |
Most nocturia patients tolerate desmopressin treatment without clinically significant hyponatraemia; however, the risk increases with increasing age and decreasing baseline serum sodium concentration. | 1a |
Treatment of nocturia in OAB patients with anticholinergic drugs shows reduction in nocturia episodes. | 1b |
Combination of PFMT and anticholinergics does not appear to confer additional benefit over anticholinergics alone. | 1b |
Combination of anticholinergic and desmopressin treatment appears to reduce nocturnal voided volume and time to first nocturnal void in women with nocturnal polyuria. | 1b |
Vaginal oestrogen may be beneficial in the treatment of nocturia in around 50% of women. | 1b |
Afternoon (timed) diuretic treatment with furosemide reduces nocturia episodes and nocturnal voided volume in men but no similar studies have been conducted in women. | 1b |
Assessment of clinical significance is important when evaluating trials involving treatment strategies for nocturia, as statistical significance can be achieved with small reductions in nocturia episodes. | 3 |
Recommendations | Strength rating |
Offer desmopressin treatment for nocturia secondary to nocturnal polyuria to women, following appropriate counselling regarding the potential benefits and associated risks (including hyponatraemia). | Strong |
Carefully monitor serum sodium concentration in elderly patients treated with desmopressin. Avoid prescribing desmopressin to patients with a baseline serum sodium concentration below normal range. | Strong |
Offer anticholinergic treatment for nocturia to women with urge urinary incontinence or other LUTS, following appropriate counselling regarding the potential benefits and associated risks. | Strong |
Inform women with nocturia that combination of behavioural therapy and anticholinergic drugs is unlikely to provide increased efficacy compared with either modality alone. | Weak |
Offer combination of anticholinergics and desmopressin to women with overactive bladder and nocturia secondary to nocturnal polyuria, following appropriate counselling regarding the potential benefits and associated risks. | Weak |
Offer vaginal oestrogen treatment to women with nocturia, following appropriate counselling regarding the potential benefits and associated risks. | Weak |
Offer timed diuretic treatment to women with nocturia secondary to polyuria, following appropriate counselling regarding the potential benefits and associated risks. | Weak |
4.6.4.4. Surgical management
Surgical treatment is generally reserved for those with underlying correctable LUT disorders. The effect of surgical treatments on symptoms of nocturia can be found in the relevant condition-specific sections of this guideline.
4.6.5. Follow-up
Follow-up of patients with nocturia is dependent on the underlying aetiology of this symptom and the treatment given.
4.7. Pelvic organ prolapse and lower urinary tract symptoms
4.7.1. Epidemiology, aetiology, pathophysiology
Pelvic organ prolapse is a common condition in adult women. The prevalence of POP is 3–6% when bothersome symptoms are used to characterise the condition and increases to 50% when a purely anatomical definition is used [619].
The estimated lifetime risk for POP surgery is 12.6% [620]. Parity, vaginal delivery, ageing, and obesity are the most commonly recognised risk factors [621].
Although the aetiology of POP is not fully understood, birth trauma to the levator ani complex is recognised as central to its development. In normal physiology, an intact levator ani complex functionally closes the genital hiatus surrounding the vagina, limiting the pressure gradient between the intra-abdominal and intravaginal areas. During physical activities, this reduces stress on the endopelvic fascia and its condensations (e.g., ligaments), which are crucial in securing the bladder, uterus, and rectum to their surroundings. Current aetiological concepts include widening of the levator hiatus due to birth trauma, which creates a low-pressure area in the vagina and consequently increased stress on the ligaments, fascial elements, and PFMs during physical activity. When the supporting function of the muscles and connective tissues fails, POP may develop [622]. This concept also explains the time lapse between birth trauma and occurrence of POP.
Pelvic organ prolapse and LUTS often occur simultaneously in women. In isolation, both POP and LUTS are prevalent conditions in women, although the prevalence of LUTS in women with POP exceeds that of LUTS in women without POP [619]. In a meta-analysis and SR, consistent results demonstrated a higher prevalence of OAB symptoms and UUI in patients with POP than without POP [619,623]. The observation that LUTS may improve or worsen after POP treatment suggests a link between these two entities [619]. Clinical examples include the occurrence of BOO symptoms in severe POP, and disappearance of SUI symptoms with progression of POP (and conversely the occurrence of SUI after treatment of POP) [624]. Pelvic organ prolapse is also associated with symptoms of bowel and/or sexual dysfunction [625].
4.7.2. Classification
Since 1996, POP has been classified according to the Pelvic Organ Prolapse-Quantification (POP-Q) system [626]. For specifics on how to perform the POP-Q measurement and the nine standard points to be measured (Figures 2 and 3), we refer to the original publications [626,627].
The vagina is divided into anterior (bladder), posterior (rectum) and apical (cervix or vaginal vault) compartments. After scoring the position of the nine POP-Q points, a prolapse of each compartment is graded numerically from stage 0 to 4, with stage 0 being no prolapse and stage 4 being complete eversion of the compartment. A crucial marker in staging POP is the hymenal remnant. Any POP with a maximum descent that is still 1 cm above the hymen (e.g., in the vagina) is considered a stage 1 POP. A maximum descent between 1 cm above and 1 cm below (outside the vagina) the hymen is a stage 2 POP. Any descent beyond 1 cm below the hymen is a stage 3 POP.
The figures below show the POP-Q staging in comparison to the Baden–Walker system (and others) used before the international consensus on the POP-Q staging was introduced as the new standard.
Figure 2: Prolapse classification system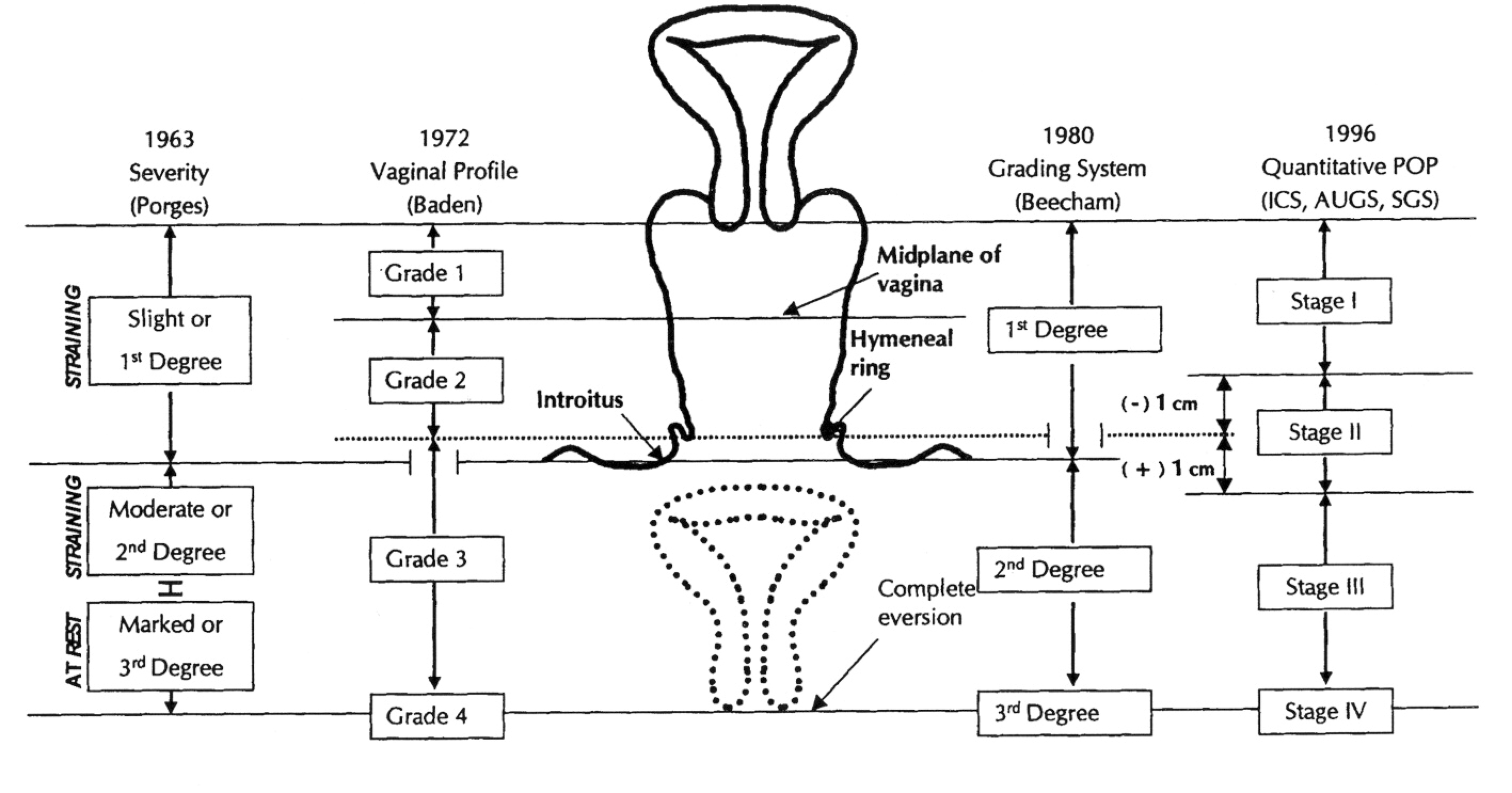 Figure reproduced with permission from the publisher, from Theofratus et al. .627
Figure reproduced with permission from the publisher, from Theofratus et al. .627
Figure: 3: Pelvic Organ Prolapse-Quantification staging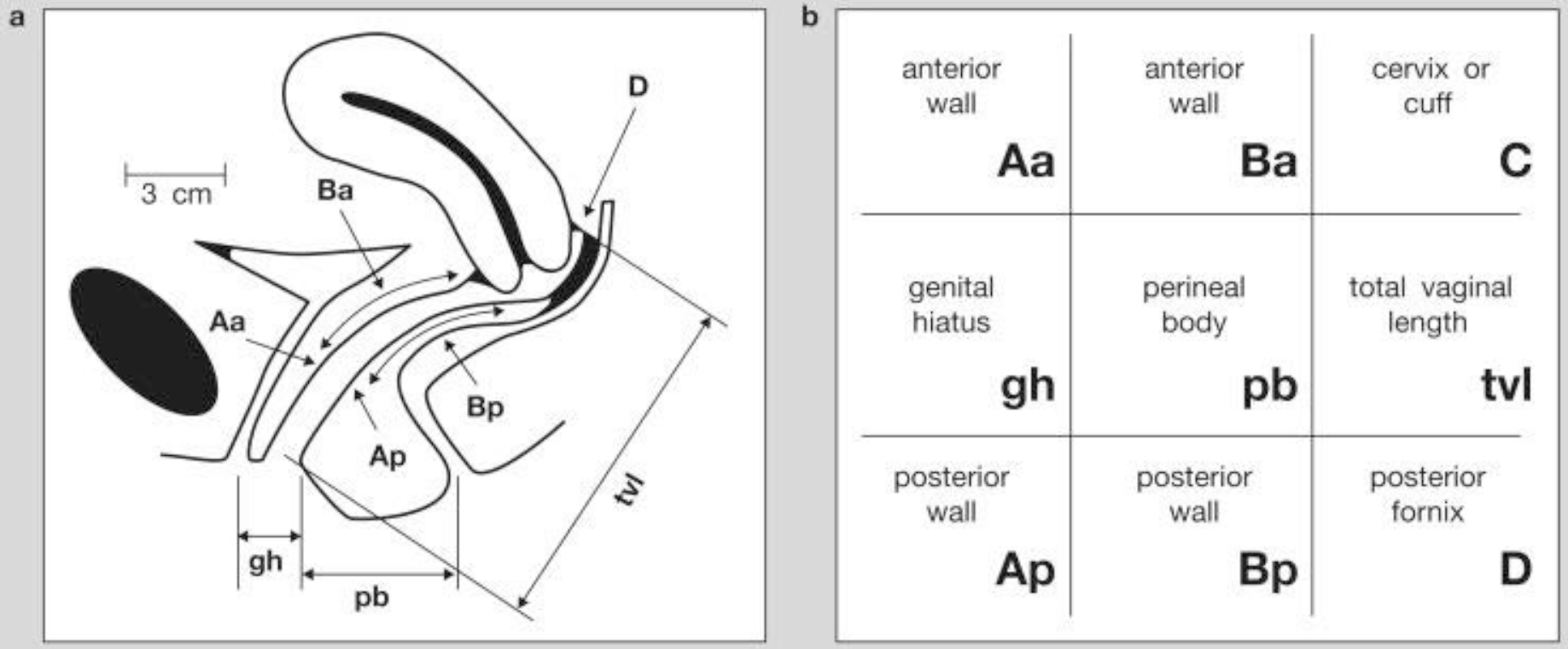 Figure reproduced with permission from the publisher, from Bump et al. . The standardisation of terminology of female POP and pelvic floor dysfunction.626
Figure reproduced with permission from the publisher, from Bump et al. . The standardisation of terminology of female POP and pelvic floor dysfunction.626
4.7.3. Diagnostic evaluation
Pelvic organ prolapse is a clinical diagnosis and is staged according to the POP-Q system. Pelvic organ prolapse that is above the hymen should only produce mild symptoms at most [628]. In cases where there is a discrepancy between the clinical symptoms and POP-Q staging, it is advised to consider performing the POP-Q measurement in a standing rather than supine position or re-evaluating at a later time in the day. Magnetic resonance imaging assessment demonstrated a marked difference in POP staging between supine and standing position [629]. Additional diagnostic tests for POP are mainly indicated if there are accompanying symptoms like LUTS or bowel dysfunction. Imaging techniques are not advised for the routine diagnostic work-up of patients presenting with POP [66]. The role of urodynamics in the diagnostic work-up of SUI has been discussed in Section 4.2, of this guideline.
The use of techniques to reduce POP during urodynamic evaluation to diagnose occult SUI is common practice. This information may be used to decide if additional anti-UI surgery should be offered at the time of POP surgery or to counsel patients on the possible after-effects of POP treatment.
There are several POP reduction methods that may be used during physical examination or urodynamic evaluation. In a multicentre observational study, five different cough/stress tests were compared for their ability to detect SUI in women with POP [630]. Stress urinary incontinence during at least one of the five tests occurred in 60/205 (29.2%) women without SUI symptoms. Looking at single test performance, the detection rate of occult SUI in women without symptoms increased from 4.4% in case of no reduction to 22% in case of reduction with a pessary.
A large RCT included women with POP without symptoms of SUI, who were randomised to sacro-colpopexy with or without Burch colposuspension [631]. Three hundred and twenty-two stress-continent women with stages 2–4 prolapse underwent standardised urodynamic testing, and the protocol included five prolapse reduction methods. Preoperatively, twelve of 313 (3.7%) women demonstrated urodynamic SUI without prolapse reduction. Preoperative detection of urodynamic SUI with prolapse reduction at 300 mL was by pessary, 6% (5/88); manual, 16% (19/122); forceps, 21% (21/98); swab, 20% (32/158); and speculum, 30% (35/118). Another large trial included women with POP without SUI symptoms randomised to vaginal POP surgery with or without (sham incision) MUS [632]. Before surgery, 33.5% (111/331) of women demonstrated SUI at a prolapse-reduction cough stress test. In an observational study of 172 women with POP without SUI, 19% of women were diagnosed with occult SUI by basic office evaluation (with prolapse reduction with swab on forceps) and 29% on urodynamic evaluation [633].
In summary, SUI can be demonstrated in women with POP without symptoms of SUI after POP reduction in up to 30% of cases. There is no consensus on the best reduction technique.
Although the detection rate of occult SUI increases after reduction of POP in women without SUI symptoms, its clinical value is under debate.
In one trial, preoperative stress-continent women were evaluated during urodynamic testing with prolapse reduction to determine if they were more likely to report postoperative SUI, regardless of concomitant colposuspension (controls 58% vs. 38% and Burch colposuspension 32% vs. 21%) [631]. In another trial, women with SUI during the cough stress test after POP reduction reported UI at three months in 29.6% in the synthetic MUS group, compared with 71.9% in the sham group [632]. Women with a positive prolapse reduction stress test before surgery appeared to receive more benefit from a synthetic MUS at three months, but not at twelve months, than did those with a negative test.
In a large observational study, women did not receive additional anti-UI surgery even if they had SUI after POP reduction preoperatively. In this scenario, 9% (16/172) of women developed postoperative de novo SUI and six underwent surgery for de novo SUI [633]. Women with demonstrable preoperative SUI were more at risk of postoperative SUI: 28% vs. 5%. Based on urodynamic evaluation only, one more woman was predicted to have postoperative SUI, but all six women who underwent treatment for de novo SUI showed SUI during basic office evaluation.
In a model developed to predict the risk of de novo SUI in women undergoing POP surgery based on findings from two trials, twelve preoperative predictors were tested [634]. Positive SUI during a preoperative prolapse reduction test was included in this model, but it failed to be a significant predictor as a single item. Preoperative POP stage was not associated with risk of de novo SUI.
4.7.3.1. Summary of evidence and recommendation for detection of SUI in women with POP
Summary of evidence | LE |
Pelvic organ prolapse reduction during cough stress test, in office or during urodynamics detects SUI in ~30% of continent women. | 2a |
Women with SUI after POP reduction preoperatively (occult SUI) is likely to be at increased risk of developing SUI symptoms after POP surgery. | 2a |
Recommendation | Strength rating |
Perform pelvic organ prolapse (POP) reduction test in continent women to identify those with occult stress urinary incontinence and counsel them about the pros and cons of additional anti-incontinence surgery at the time of POP surgery. | Strong |
4.7.3.2. Urodynamics in women with pelvic organ prolapse and LUTS (without stress urinary incontinence)
The role of urodynamics is less clear in women presenting with POP and concurrent LUTS, other than SUI. Pelvic organ prolapse is a complex condition incorporating different compartments of the vagina and presenting at different stages of severity. Information about detrusor activity, as assessed with urodynamics, may provide information about the risk of developing DO after surgery, but also on the risk of urinary retention due to DU. An observational study assessed predictors for DO following POP surgery for POP-Q stage 3 or higher in 1,503 women and the authors concluded that preoperative maximum urethral closure pressure > 60 cm H2O, Qmax < 15 mL/s, maximum detrusor voiding pressure (Dmax) > 20 cm H2O and PVR volume > 200 mL were independent risk factors for postoperative DO [635]. A small observational study (n = 49) evaluated patients with preoperative DU (detrusor pressure at maximum flow was < 10 cm H2O and Qmax < 12 mL/s) after POP surgery. Surgery objectively cured DU in 47% of women and urodynamic findings normalised after surgery [636]. The 2019 NICE Guidelines do not include a recommendation to perform urodynamics as part of the diagnostic work-up of POP, except for combination with symptomatic SUI [66].
4.7.4. Disease management
Pelvic organ prolapse symptoms can be treated with PFMT, vaginal pessary, surgery, or a combination of these treatments. The scope of these guidelines is to focus on LUTS in women; therefore, only data on the effect of treatment of urinary symptoms are presented.
4.7.4.1. Conservative management of pelvic organ prolapse
The 2013 NICE guidelines on Urinary Incontinence and POP in Women had an updated management section in 2019, including a full evidence review [66]. The overall conclusion with respect to conservative treatment for POP was that the evidence is of low quality. Thirteen RCTs were identified. Seven studies presented data on changes in urinary symptoms [637-643]. An additional search identified four RCTs that addressed the addition of PFMT to POP surgery [644-647], and one that compared combined PFMT/Pilates therapy with lifestyle advice by leaflet [648].
Five studies [638,640-642,648] compared PFMT to lifestyle advice/leaflet; one study [639] compared PFMT alone to PFMT with pessary; one study [643] compared PFMT to pessary therapy; and five studies compared surgery for POP with or without addition of PFMT [637,644-647].
4.7.4.1.1. Pelvic floor muscle training versus lifestyle advice
An RCT (n = 109) reported that, at six months’ follow-up, the ICIQ-UI-SF scores improved in favour of the PFMT group (2.40 points) compared with a control group receiving lifestyle advice only (0.2 points), but the mean baseline score in the PFMT group was higher than in the control group (7.4 vs. 5.9) [638]. Likewise, it has to be noted that the absolute ICIQ-UI-SF values at six months’ follow-up were not significantly different between PFMT (4.8) and controls (5.2).
Two publications from one RCT reported on the three-, six- and twelve-month results of lifestyle advice only vs. lifestyle advice combined with group PFMT [640,641]. The Urogenital Distress Inventory-6 (UDI-6) and Urinary Impact Questionnaire-7 (UIQ-7) questionnaires were used to assess urinary symptoms. At three months’ follow-up, both groups (53 women in the lifestyle group and 56 in the lifestyle + PFMT cohort) reported significantly improved UDI-6 scores, while the lifestyle-only group also reported significantly greater improvement in the UIQ-7 score. Between-group comparison showed no differences in UDI-6 and UIQ-7 scores at six months. At twelve months’ follow-up, the majority of women had sought additional treatment (70% in the lifestyle-only group and 48% in the lifestyle/PFMT group). The number of patients remaining on the original therapy was too small to reach strong conclusions.
One RCT reported on six- and twelve-months follow-up of 225 women with POP-Q stage 1–3 randomised to individualised PFMT and 222 women randomised to lifestyle leaflet information only (control) [642]. At six months, significantly more women in the control group reported UI, the need to strain to empty their bladder, and the feeling of incomplete emptying compared to the PFMT group. ICIQ-SF score was also significantly worse in the control group as compared to the PFMT group. However, at twelve months, there was no significant difference in these items between groups. It has to be noted that 50% in the control group received additional treatment within the twelve-month study period. Twenty-seven percent had additional PFMT, which may have had an effect on the twelve-month data.
Another RCT reported on the 24-month follow-up of 414 women with stage 1–3 POP (207 assigned to PFMT/Pilates and 207 to lifestyle advice) [648]. Urinary symptoms were assessed with the ICIQ-UI-SF and a question about UI and difficulty emptying the bladder. At 24 months, the ICIQ-UI-SF score was significantly better in the intervention group (mean difference –0.83). However, the proportion of women reporting any UI did not differ between the groups, nor did the number of pads used weekly.
One RCT compared PFMT alone to PFMT and pessary for symptomatic POP [639]. Urinary tract symptom changes were assessed using UDI-6 and UIQ at six and twelve months follow-up. At twelve months, there was no difference in the between-group comparison. With respect to the UIQ, women in the pessary/PFMT group showed a significant improvement from baseline, but the PFMT-only group did not. Women in the pessary/PFMT group reported significantly more frequent de novo SUI (48% vs. 22%), and more improvement of pre-existing voiding difficulty (62.5% vs. 35.5%).
4.7.4.1.2. Pelvic floor muscle training versus pessary only
One RCT reported on the 24-month follow-up of 82 women with symptomatic POP randomised to pessary therapy and 80 women randomised to PFMT [649]. Both in the ITT and per protocol analyses, the UDI-6 score did not differ significantly between groups at 24 months of follow-up.
4.7.4.1.3. Surgery alone versus surgery with pelvic floor muscle training
An assessor blinded RCT compared surgery for POP with or without additional pre-and postoperative PFMT. At twelve months after surgery, there were no significant differences between the groups on the change in scores of the UDI nor the IIQ scores [637].
Another RCT reported on the six-month follow-up of 57 women (28 surgery/29 surgery with PFMT). There was a significant improvement in the UDI-6 score for both groups, but not between groups [645].
Another RCT reported on the results of a 2x2 factorial design in which women were first randomised between two surgical techniques for POP and between additional PFMT (n = 188) or not (n = 186) [646]. The UDI was used to assess urinary symptoms up to 24 months. No significant differences were found between the addition of PFMT to surgery or not. Another study of the same population reported on SUI in particular [647]. No significant differences were found between women who had additional PFMT and those who had not.
In 2020 an RCT reported on 40- and 90-days follow-up of 48 women randomised to supervised PFMT before and after surgery and 40 women having surgery only [644]. No significant differences in UDI-6 scores were identified at 40 and 90 days.
ICI 2017 [18] concluded that there is level 1a evidence that PFMT reduces pelvic floor symptoms in women with POP, there is some evidence that it reduces POP specific symptoms like bulging. Some RCTs also show an improvement in POP stage with PFMT [650]. The NICE guidelines on the management of POP advocate considering supervised PFMT for > 16 weeks as initial treatment for symptomatic prolapse [66]. The use of pessary is also to be considered, alone or combined with PFMT. It is important to recognise that a benefit is expected on typical POP symptoms, like feeling or seeing a bulge out of the vagina, and not on LUTS, as the reported RCTs showed. From a urological perspective, initiating conservative treatment for asymptomatic POP in order to treat UI or bladder emptying problems is not supported by the data.
4.7.4.1.4. Pessary versus surgery alone
A prospective cohort study showed that surgery in comparison with pessary treatment resulted in statistically significant more women reporting subjective improvement [651].
4.7.4.1.5. Summary of evidence and recommendation for the conservative treatment of pelvic organ prolapse and lower urinary tract symptoms
Summary of evidence | LE |
Pelvic floor muscle training improves LUTS for up to 6 months in POP patients who do not have additional pessary or surgical treatment. | 2a |
If pessary therapy or surgical intervention is used for POP, PFMT does not show an additional benefit. | 2a |
Recommendations | Strength rating |
Inform women with pelvic organ prolapse (POP), who do not need a vaginal pessary or surgical intervention, about the potential relief from lower urinary tract symptoms (LUTS) from pelvic floor muscle training (PFMT). | Strong |
Do not offer preoperative PFMT to improve outcome of LUTS if pessary therapy or surgical intervention is indicated for POP. | Strong |
4.7.4.2. Pelvic organ prolapse surgery and overactive bladder
Only a few studies have specifically addressed the effect of POP surgery on OAB symptoms. A SR of twelve studies, excluding women with SUI, evaluated OAB symptoms before and after surgery [623]. All but one study reported improvement of OAB symptoms. The same authors performed a prospective analysis of 505 women who had POP surgery with or without mesh [652]. Mean follow-up was 12.7 months. The incidence of bothersome urinary frequency reduced from 36.6% to 14.6%, with de novo symptoms occurring in 6.1%. Bothersome urgency symptoms reduced in 36.8% to 12.9% of women, with 5.0% developing de novo symptoms. Urge urinary incontinence symptoms reduced from 21.2% to 6.1% of women, with 5.3% developing de novo symptoms.
One observational study evaluated frequency and urgency symptoms without consideration of bother in 87 women undergoing POP surgery and showed an improvement in frequency by 75%, and in urgency in 83% [653]. The effect of the POP-Q stage did not seem to influence the effect of surgery on OAB symptoms [652,653].
Another observational study (n = 43) evaluated the effect of posterior repair on OAB/DO and showed a 70–75% improvement rate in both parameters after surgery [654].
4.7.4.3. Pelvic organ prolapse surgery and bladder outlet obstruction
The criteria for BOO are based on urodynamic assessment. POP can be categorised as anatomical BOO, which is addressed in Sections 4.5.2.2 and 4.5.3.1.
4.7.4.4. Pelvic organ prolapse surgery and stress urinary incontinence
The aim of this section is to address the options available to women who require surgery for POP and who have associated SUI (either before or after reduction of prolapse), and to assess the value of prophylactic anti-UI surgery in women with no evidence of SUI.
A SR and meta-analysis of ten trials on prolapse surgery with or without an anti-incontinence procedure was reported in 2018 [655]. In addition, a Cochrane review including nineteen trials (n = 2,717) evaluating bladder function after surgery for POP presented analyses of women with POP and SUI, women with POP and occult SUI, and women with POP who were continent [656].
4.7.4.4.1. Vaginal pelvic organ prolapse surgery in women with stress urinary incontinence
Two trials addressed postoperative SUI in patients who had been diagnosed with SUI preoperatively and had vaginal POP surgery [657,658]. Two trials (n = 185 and 134) compared the use of MUS at initial POP surgery to POP surgery alone. The RR for postoperative SUI was 0.30 in favour of the combined POP surgery and MUS group. One of these two trials also compared the use of MUS at initial POP surgery and at three months if SUI persisted [657]. At twelve months’ follow-up, there was no difference between the groups regarding postoperative UI (RR 0.41); however, 44% of the women without initial MUS never required surgery and 29% were dry.
4.7.4.4.2. Abdominal pelvic organ prolapse surgery in women with stress urinary incontinence
One RCT randomised 47 women with POP and SUI to an abdominal POP surgical procedure, e.g., sacro-colpopexy with or without Burch colposuspension. Additional SUI surgery did not improve postoperative SUI as compared to sacro-colpopexy alone (RR: 1.38) [659]. This finding remained consistent over five years’ follow-up [660]. Another RCT compared the addition of a MUS or Burch colposuspension to an abdominal sacro-colpopexy in 113 women with POP and SUI [661]. At two years’ follow-up, the RR for postoperative SUI was 0.54 in favour of the MUS group.
4.7.4.5. Vaginal pelvic organ prolapse surgery in continent women
One RCT compared vaginal POP surgery alone with concomitant POP surgery and MUS in 220 women. Postoperative SUI occurred in 46/113 (40.7%) women who had POP surgery alone, compared to 30/107 (28.0%) who had additional MUS (RR: 0.69) [656].
4.7.4.5.1. Abdominal pelvic organ prolapse surgery in continent women
Two RCTs compared abdominal sacro-colpopexy with (n = 180) or without (n = 187) Burch colposuspension with an outcome favouring the addition of Burch colposuspension (RR for de novo SUI: 0.69) [659,662]. However, 34% of women in the prophylactic Burch colposuspension group developed de novo SUI (as compared to 49% in the control group). An RCT with medium-term follow-up (mean 39.5 months) showed that additional SUI surgery was needed by only 1/31 women (3%) in both groups [660,663].
4.7.4.5.2. Vaginal pelvic organ prolapse surgery in women with prolapse and occult stress urinary incontinence
Five RCTs including a total of 194 women who had vaginal POP repair alone and 174 women who had an additional MUS at the time of primary surgery were identified [632,664-667]. The RR of postoperative SUI was 0.38 in favour of the MUS group.
4.7.4.6. Adverse events associated with combined pelvic organ prolapse and stress urinary incontinence surgery
Data from six RCTs on vaginal POP surgery with MUS were pooled to assess adverse events [632,657,658,665-667]. Urgency urinary incontinence was less frequent after combination surgery as compared to POP surgery alone (28% vs. 42%; RR: 0.7), but there was a tendency towards more voiding problems. Adverse events directly related to surgery occurred more often in the combination group (28% vs. 15%; RR: 1.8), as did serious adverse events such as bladder perforation, urethral injuries, and tape exposure (14% vs. 8%; RR: 1.7) [655].
In summary, it is difficult to generalise the results of trials using different procedures to treat both POP and UI. It seems that with a combined procedure, the rate of postoperative SUI is lower but voiding symptoms and complication rates are higher. Studies using MUS have shown more significant differences in UI outcomes with combined procedures than when other types of anti-UI procedure have been used. It must be taken into account that although more women are dry after combined surgery for POP with MUS, there are potential adverse events that should be balanced against potential benefits.
4.7.5. Summary of evidence and recommendations for surgery in women with both pelvic organ prolapse and stress urinary incontinence
Summary of evidence | LE |
Women with POP and UI | |
Surgery for POP and SUI shows a higher rate of cure of UI in the short-term than POP surgery alone. | 1a |
There is conflicting evidence on the relative long-term benefit of surgery for POP and SUI vs. POP surgery alone. | 1a |
Combined surgery for POP + SUI carries a higher risk of adverse events than POP surgery alone. | 1a |
Continent women with POP | |
Continent women with POP are at risk of developing SUI postoperatively. | 1a |
Women with POP and OAB | |
There is some low-level inconsistent evidence to suggest that surgical repair of POP can improve symptoms of OAB. | 2b |
Recommendations for women requiring surgery for bothersome pelvic organ prolapse (POP) who have symptomatic or occult stress urinary incontinence (SUI) | Strength rating |
Offer simultaneous surgery for POP and SUI only after a full discussion of the potential risks and benefits of combined surgery vs. POP surgery alone. | Strong |
Inform women of the increased risk of adverse events with combined prolapse and anti-urinary incontinence surgery compared to prolapse surgery alone. | Strong |
Recommendations for women requiring surgery for bothersome POP who do not have | |
Inform women that there is a risk of developing de novo SUI after prolapse surgery. | Strong |
Do not offer concomitant anti-incontinence surgery at the time of abdominal prolapse surgery. | Strong |
4.8. Urinary fistula
The evidence relating to diagnosis and treatment of urinary fistulae is generally low level and largely composed of case series and other consensus statements. In particular, the epidemiology, aetiology, diagnosis, treatment and prevention of obstetric and non-obstetric fistulae have been described in detail during the 2016 ICI conference [668]. Most non-obstetric fistulae are iatrogenic in origin, caused by pelvic surgery (e.g., hysterectomy for benign or malignant conditions, bowel resection, and urological surgery). The risks during pelvic surgery increase proportionally to the complexity of the resection, the extent of the primary disease, and with a past history of radiotherapy (especially for recurrent disease). When a fistula occurs following radiotherapy for primary treatment, this may be an indication of tumour recurrence.
4.8.1. Epidemiology, aetiology and pathophysiology
4.8.1.1. Obstetric fistula
According to the WHO, fistulae affect > 2 million women, mostly from sub-Saharan African and Asian countries. The pooled prevalence of fistula from population studies is 0.29/1000 pregnancies [669]. Poor quality obstetric care, staff unaccountability, late referral, and poor nursing standards have been identified as health system causes [669]. However, obstructed labour is poorly documented. The main individual risk factors include age at first marriage, short stature, pregnancy with a male child, failure to attend antenatal care, low socio-economic status, low social class, lack of employment, and illiteracy [670-672]. Obstetric fistulae have detrimental consequences on global and individual health and are associated with malnutrition, sexual dysfunction, anxiety, depression, insomnia, social isolation, worsening poverty, and suicide [673,674].
4.8.1.2. Iatrogenic fistula
Poor obstetric care is usually responsible for VVFs in the developing world. By contrast, in the developed world, gynaecological or pelvic surgery is the main cause of VVF. In a recent French epidemiological study, pelvic surgery accounted for two thirds of VVF causes [675].
4.8.1.2.1. Post-gynaecological surgery
An injury to the urinary tract during hysterectomy for benign conditions (60–75%), hysterectomy for malignant conditions (30%) and caesarean section (6%) are the main causes of postoperative VVF in the developed world [676,677]. The risk of pelvic organ fistula following hysterectomy ranges from 0.1-4% [678].
Fistulae may also occur as a result of primary or recurrent malignancy, or as a consequence of cancer treatment by surgery, radiotherapy, and/or chemotherapy.
In a study including 536 women undergoing radical hysterectomy for invasive cervical cancer, bladder injury occurred in 1.5% with VVFs forming in 2.6% and uretero-vaginal fistulae (UVFs) in 2.4% of cases [679]. Overall, the rate of urogenital fistula appears to be ~9 times higher following radical hysterectomy for malignant disease as compared to that following simple hysterectomy (abdominal or vaginal for benign conditions) [680]. Bladder-sparing techniques during pelvic exenteration can increase the risk of fistula formation [681].
4.8.1.2.2. Radiation fistula
The risk of fistula seems to be higher for postoperative external beam radiation (1.9%) compared to intravaginal brachytherapy (0.8%) [682], without any predictive factor being identified [683]. This is most likely due to the heterogeneity of data regarding the tumour type and stage, the form of radiation, and the site and dose delivered.
4.8.1.2.3. Rare causes of vesico-vaginal fistula
Foreign bodies such as pessaries, sex toys, cups etc. can be a cause of delayed presentation of VVF [684-686]. Ketamine abuse has also been shown to be responsible for fistula formation [687].
4.8.1.3. Summary of evidence for epidemiology, aetiology, and pathophysiology of urinary fistula
Summary of evidence | LE |
The risk of injury to the urinary tract and subsequent fistula formation is higher in women with malignant disease undergoing radical surgery than in women with benign disease undergoing simple surgical procedures. | 2 |
The rate of fistula formation following external beam radiotherapy for gynaecological cancer appears to be of the same order as that following surgical treatment. | 4 |
4.8.2. Classification
Due to the plethora of VVF classification systems, a consensual classification system needs to be adopted. The Waaldijk and Goh classifications are widely used for diagnosis and follow-up [688-690] but were originally designed for obstetric fistulae and their use in iatrogenic fistulae is less relevant [691]. Waaldijk’s classification is based on the size and site of the fistulae and divides them into three main categories: type 1 are VVFs with no urethral involvement; type 2 are those that involve the urethra (and are sub-classified into those with circumferential and non-circumferential urethral involvement); and type 3 are fistulae involving other parts of the urinary tract. Goh’s classification also uses the presence or absence of urethral involvement to sub-categorise VVFs and considers the degrees of fibrosis present. The WHO classification (Table 6) was originally developed for obstetric fistulae and separates fistulae into simple and complex.
Table 6: Adapted WHO Classification of fistulae [669]*
Simple fistula with good prognosis | Complex fistula with uncertain prognosis |
|
|
*Although this classification was developed for obstetric fistula initially, it could be relevant for iatrogenic fistula as well.
4.8.2.1. Recommendation for the classification of urinary fistula
Recommendation | Strength rating |
Use a classification system for urinary tract fistulae to try to standardise terminology in this subject area. | Strong |
4.8.3. Diagnostic evaluation
Leakage of urine is the hallmark sign of a urogenital fistula. The leakage is usually painless, may be intermittent if it is position dependent, but more usually is constant. Unfortunately, intraoperative diagnosis of a genito-urinary or gastrointestinal injury is made in only about half of the cases [692]. Diagnosis of VVF usually requires clinical assessment often in combination with appropriate imaging or laboratory studies. As for any LUTS, history taking and focused physical examination with direct visual inspection are essential parts of urinary fistula diagnostic evaluation. Cystoscopy and retrograde bladder filling with a coloured fluid with placement of a tampon into the vagina to identify staining facilitate diagnosis of VVF. A double-dye test to differentiate between UVF and VVF may be useful in some cases [677]. Testing the creatinine level in either the extravasated or collected fluid will confirm fluid leakage as urine. Contrast-enhanced CT with late excretory phase reliably diagnoses urinary fistulae and provides information about ureteric integrity and the possible presence of associated urinoma. Magnetic resonance imaging, in particular with T2 weighting, also provides diagnostic information regarding fistulae [693].
Summary of evidence | LE |
As for any LUTS, history taking and focused physical examination with direct visual inspection are essential parts of urinary fistula diagnostic evaluation. | 3 |
Cystoscopy and retrograde bladder filling with a coloured fluid with placement of a tampon into the vagina to identify staining facilitate diagnosis of VVF. | 3 |
Contrast-enhanced CT with late excretory phase reliably diagnoses urinary fistulae and provides information about ureteric integrity. | 3 |
Magnetic resonance imaging, in particular with T2 weighting, also provides diagnostic information regarding fistulae. | 3 |
Recommendations | Strength rating |
Take a complete medical history and perform a focused physical examination including direct visual inspection for evaluation of women with suspicion of urinary fistula. | Strong |
Use cystoscopy and retrograde bladder filling with a coloured fluid to confirm the diagnosis of urinary fistula. | Weak |
Contrast-enhanced CT with late excretory phase and magnetic resonance imaging can be used in cases where the diagnosis of urinary fistula is challenging or to provide additional diagnostic information. | Weak |
4.8.4. Management of fistula
4.8.4.1. Management of vesico-vaginal fistula
4.8.4.1.1. Conservative management
4.8.4.1.1.1. Spontaneous closure
The reported spontaneous closure rate is 13 ± 23% [694], although this applies largely to small fistulae (< 1 cm) [668,695]. Hence, immediate management is usually by urinary catheterisation or diversion; however, within the first two weeks following fistula occurrence, delayed surgical exploration and repair can be planned.
4.8.4.1.1.2. Pharmacotherapy
Several case reports describe a successful fistula closure rate following the induction of amenorrhoea by oestrogen, oestrogen/progesterone combinations or luteinising hormone releasing hormone analogues specifically for small (< 7 mm), uretero- or vesico-uterine fistulae following caesarean section [696-702]. One RCT comparing the efficacy of using fibrin glue compared to Martius flap inter-positioning (n = 14; < 4 cm and n = 5; > 5 cm) did not report significantly different outcomes between the two types of treatment but the closure rates were relatively low in both groups (68.4% vs. 57.9%) [703].
4.8.4.1.1.3. Palliation and skin care
During the intervening period between diagnosis and repair, UI pads with the aim of prevention of skin complications related to chronic urinary leakage can be provided and the use of a barrier cream or local oestrogen can also be considered [704,705].
4.8.4.1.2. Surgical management
Overall closure rates after surgical repair of vesico-vaginal fistulae range from 58-100% [706].
4.8.4.1.2.1. Timing of surgery
Findings from small uncontrolled case series suggest no difference in success rates for early (within four weeks) or delayed (after three months) closure of VVF [707,708].
4.8.4.1.2.2. Surgical approaches
Vaginal procedures
There are two main types of closure techniques applied to the repair of urinary fistulae, the classical saucerisation/partial colpocleisis [694] and the more commonly used dissection and repair in layers or flap-splitting technique [709]. There are no data comparing their outcomes.
Abdominal procedures
There are no RCTs comparing abdominal and vaginal approaches. Repair by the abdominal route is indicated when high fistulae are fixed at the vaginal vault and are inaccessible via a vaginal approach. A transvesical repair has the advantage of being entirely extraperitoneal. A simple transperitoneal repair is used less often although it is favoured by some using the laparoscopic approach. A combined transperitoneal and transvesical procedure may be utilised for fistula repair following caesarean section. Results of secondary and subsequent repairs are not as successful as the initial repair [710].
Laparoscopic and robotic procedures
Small series (single figures) have reported using these techniques, but while laparoscopic repair is feasible with and without robotic assistance, no series to date have compared outcomes with alternative surgical approaches.
Trimming of fistula edge
A single RCT compared trimming of the fistula edge with no trimming. There was no difference in success rates but failed repairs in trimmed cases had larger recurrences than untrimmed cases, which were smaller [711].
Tissue interposition
Tissue flaps are often added as an additional layer of repair during VVF surgery. Most commonly, such flaps are utilised in the setting of recurrence after a prior attempt at repair, for VVF related to previous radiotherapy (described later), ischaemic or obstetric fistulae, large fistulae, and finally those associated with a difficult or tenuous closure due to poor tissue quality. However, there is no high-level evidence that the use of such flaps improves outcomes for either complicated or uncomplicated VVF.
Postoperative management
There is no high-level evidence to support any particular practice in postoperative management, but most reported series used catheter drainage for > 10 days and longer periods in complex or radiation-associated fistulae (up to three weeks). The performance of postoperative cystography prior to catheter removal can theoretically miss a persistent fistula if not done with a micturition phase or if the fistula is located at the bladder neck.
4.8.4.1.3. Management of complications of vesico-vaginal fistulae
The complications of VVF repair are varied and can include:
- Persistence or recurrence of fistula;
- Persistence or recurrence of UI;
- Persistence of LUTS or occurrence of new LUTS, including de novo OAB and/or SUI;
- Infections: wound and UTIs/urosepsis;
- Ureteric obstruction (ligation, fibrosis or injury);
- Bladder outlet obstruction (meatal stenosis, urethral stricture or bladder neck obstruction);
- Bladder contracture;
- Vaginal stenosis;
- Sexual dysfunction (vaginismus/dyspareunia);
- Rare complications (granulomas/diverticulum formation);
- Neurological complications (foot drop/neurogenic bladder);
- Psychological trauma (social isolation/divorce/mental illness);
- Infertility.
The literature on the treatment and management of complications of fistula repairs is scarce and is mostly experienced based. It is impossible to provide any specific evidence-based guidance.
4.8.4.2. Management of radiation fistulae
Modified surgical techniques are often required, and indeed, where the same techniques have been applied to both surgical and post-radiation fistulae, the results from the latter have been consistently poorer [712]. Due to the wide field abnormality surrounding many radiotherapy-associated fistulae, approaches include permanent urinary and/or faecal diversion [712,713] or preliminary urinary and faecal diversion, with later undiversion in selected cases following reconstruction. In cases where life expectancy is deemed to be short, ureteric occlusion and nephrostomy insertion might be more appropriate.
4.8.4.3. Management of ureteric fistulae
Patients at higher risk of ureteric injury require experienced surgeons who can identify and protect the ureter and its blood supply to prevent injury and recognise injury promptly. Immediate repair of any intraoperative injury should be performed by observing the principles of debridement, adequate blood supply and tension-free anastomosis with internal drainage using stents [714]. Delayed presentation of UUT injury should be suspected in patients whose recovery after relevant abdominal or pelvic surgery is slower than expected, if there is any fluid leak, and if there is any unexpected dilatation of the pelvicalyceal system.
While there is no evidence to support the use of one surgical approach over another, there is consensus that repair should adhere to the standard principles of tissue repair and safe anastomosis and be undertaken by an experienced team. Conservative management is possible with internal or external drainage, endoluminal management using nephrostomy and stenting where available, and early (< 2 weeks) or delayed (> 3 months) surgical repair when required [715]. Functional and anatomical imaging should be used to follow-up patients after repair to guard against development of ureteric stricture and deterioration in renal function.
Uretero-vaginal fistula occurring in the early postoperative phase predominantly after hysterectomy is the most frequent presentation of UUT fistulae in urological practice. An RCT in 3,141 women undergoing open or laparoscopic gynaecological surgery found that prophylactic insertion of ureteric stents made no difference to the low risk (1%) of ureteric injury [716].
Endoscopic management is sometimes possible by retrograde stenting, percutaneous nephrostomy and antegrade stenting if there is pelvicalyceal dilatation, or ureteroscopic realignment [717]. However, the long-term success rate is unknown. Antegrade endoluminal distal ureteric occlusion combined with nephrostomy tube diversion often palliates urinary leakage due to malignant fistula in the terminal phase [718]. If endoluminal techniques fail or result in secondary stricture, the abdominal approach to repair is standard and may require end-to-end anastomosis, reimplantation into the bladder using psoas hitch or Boari flap, or replacement with bowel segments with or without reconfiguration. As a last resort, nephrectomy may be considered, particularly in the context of a poorly functioning kidney and an otherwise normal contralateral kidney [719-723].
4.8.4.3.1. Management of urethro-vaginal fistulae
4.8.4.3.1.1. Aetiology
Although urethro-vaginal fistulae are rare, most of them in adults have an iatrogenic aetiology. Causes include surgical treatment of SUI with bulking agents or synthetic slings, surgery for urethral diverticulum and genital reconstruction. Irradiation and even conservative treatment of prolapse with pessaries can lead to formation of fistulae.
4.8.4.3.1.2. Diagnostic evaluation
Clinical vaginal examination, including the three-swab test, is often sufficient to diagnose urethro-vaginal fistulae. Urethroscopy and cystoscopy can be performed to assess the extent and location of the fistulae. In cases of difficult diagnosis, VCUG or US can be useful. An 3D-MRI or CT scan is becoming utilised more widely to clarify anatomy [724,725].
4.8.4.3.1.3. Surgical management
Choice of surgery will depend on the size, localisation, and aetiology of the fistula and the amount of tissue loss. Principles of reconstruction include identifying the fistula, creation of a plane between the vaginal wall and urethra, watertight closure of the urethral wall, eventual interposition of tissue, and closure of the vaginal wall.
One case series reported that a vaginal approach yielded a success rate of 70% at first attempt and 92% at second attempt, and that an abdominal approach only led to successful closure in 58% of cases [726]. A vaginal approach required less operating time, had less blood loss and shorter hospitalisation.
Most authors have described surgical principles that are identical to those of VVF repair, and primary closure rates of 53–95.4% have been described. A series of 71 women, treated for urethro-vaginal fistulae reported that 90.1% of fistulae were closed at the first vaginal intervention. Additionally, 7.4% were closed during a second vaginal intervention. Despite successful closure, SUI developed in 52% of cases. Stress urinary incontinence patients were treated with synthetic or autologous slings and nearly 60% became dry and an additional 32% improved. Urethral obstruction occurred in 5.6% and was managed by urethral dilation or urethrotomy [727].
4.8.4.3.1.4. Flaps and neo-urethra
The simplest flap is a vaginal advancement flap to cover the urethral suture line. Labial tissue can be harvested as a pedicled skin flap. This labial skin can be used as a patch to cover the urethral defect but can also be used to create a tubular neo-urethra [728,729]. The construction of a neo-urethra has mostly been described in traumatic aetiologies. In some cases, a transpubic approach has been used [730]. The numbers of patients reported are small and there are no data on the long-term outcome of fistula closure and continence rates. The underlying bulbo-cavernosus tissue can be incorporated in the pedicled flap and probably offers better vascularisation and more bulking to the repair. This could allow a safer placement of a sling afterwards, in those cases where bothersome SUI would occur postoperatively [731,732].
4.8.4.3.1.5. Martius flap
In obstetrical fistula repair, the Martius labial bulbocavernosus muscle/fat flap was not found to have any benefit. However, the Martius flap is still considered by some to be an important adjunctive measure in the treatment of genitourinary fistulae for which additional bulking with well-vascularised tissue is needed [733]. The series of non-obstetrical aetiology are small and all of them are retrospective. There are no prospective data, nor randomised studies [734]. The indications for Martius flap in the repair of urethra-vaginal fistulae remain unclear.
4.8.4.3.1.6. Rectus muscle flap
Rectus abdominis muscle flaps have been described by some authors [735,736].
4.8.4.3.1.7. Alternative approaches
An alternative retropubic retro-urethral technique has been described by Koriatim [737]. This approach allows a urethro-vesical flap tube to be fashioned to form a continent neo-urethra.
4.8.4.4. Summary of evidence and recommendations for the management of urinary fistula
Summary of evidence | LE |
Spontaneous closure of surgical fistulae does occur and appears more likely for small fistulae although it is not possible to establish the rate with any certainty. | 3 |
There is no evidence that the timing of repair makes a difference to the chances of successful closure of a fistula. | 3 |
There is no high-quality evidence of differing success rates for repair of VVFs by vaginal, abdominal, transvesical, and transperitoneal approaches. | 3 |
A variety of interpositional grafts can be used in either abdominal or vaginal procedures, although there is little evidence to support their benefits in any specific setting. | 3 |
Post-radiation fistula | |
Success rates are lower for irradiated fistulae than for non-radiated fistulae. | 3 |
Ureteric fistula | |
Prophylactic ureteric stent insertion does not reduce risk of ureteric injury during gynaecological surgery. | 2 |
Antegrade endoluminal distal ureteric occlusion combined with nephrostomy tube diversion often palliates urinary leakage due to malignant fistula in the terminal phase. | 4 |
Urethro-vaginal fistula | |
Urethro-vaginal fistula repair may be complicated by SUI, urethral stricture, and urethral shortening, which may necessitate long-term follow-up. | 3 |
Recommendations | Strength rating |
General | |
When reporting on outcomes after fistula repair, authors should make a clear distinction between fistula closure rates and postoperative urinary incontinence rates and the time at which the follow-up was organised. | Strong |
Do not routinely use ureteric stents as prophylaxis against injury during routine gynaecological surgery. | Strong |
Suspect ureteric injury or fistula in patients following pelvic surgery if a fluid leak or pelvicalyceal dilatation occurs postoperatively, or if drainage fluid contains high levels of creatinine. | Strong |
Use three-dimensional imaging techniques to diagnose and localise urinary fistulae, particularly in cases with negative direct visual inspection or cystoscopy. | Weak |
Manage upper urinary tract fistulae initially by conservative or endoluminal techniques where such expertise and facilities exist. | Weak |
Surgical principles | |
Surgeons involved in fistula surgery should have appropriate training, skills, and experience to select an appropriate procedure for each patient. | Weak |
Attention should be given as appropriate to skin care, nutrition, rehabilitation, counselling, and support prior to, and following, fistula repair. | Weak |
Tailor the timing of fistula repair to the individual patient and surgeon requirements once any oedema, inflammation, tissue necrosis, or infection, are resolved. | Weak |
Ensure that the bladder is continuously drained following fistula repair until healing is confirmed (expert opinion suggests: ten to fourteen days for simple and/or post-surgical fistulae; fourteen to 21 days for complex and/or post-radiation fistulae). | Weak |
Where urinary and/or faecal diversions are required, avoid using irradiated tissue for repair. | Weak |
Use interposition graft when repair of radiation associated fistulae is undertaken. | Weak |
Repair persistent urogenital fistulas by an abdominal approach using open, laparoscopic, or robotic techniques according to availability and competence. | Weak |
Urethro-vaginal fistulae should preferably be repaired by a vaginal approach. | Weak |
4.9. Urethral diverticulum
A female urethral diverticulum is a sac-like protrusion composed of the entire urethral wall or only the urethral mucosa, situated between the peri-urethral tissues and the anterior vaginal wall.
4.9.1. Epidemiology, aetiology, pathophysiology
Urethral diverticulum is an uncommon condition with an estimated prevalence of 1–6%. A prevalence of up to 10% was reported among women with LUTS attending a tertiary referral centre [738]. However, as many patients are asymptomatic or misdiagnosed, the true incidence is unknown [739-741]. Given the rarity of the condition, most published series are small and single institutional. Urethral diverticulum is thought to arise from repeated obstruction, infection, and subsequent rupture of peri-urethral glands into the urethral lumen, resulting in an epithelialised cavity that communicates with the urethra [739].
Iatrogenic damage to the urethra may also play a role, as up to 20% of women with urethral diverticula are noted to have a history of urethral surgery, dilation, or traumatic delivery [739,742]. Iatrogenic urethral diverticula formation associated with synthetic sub-urethral sling has also been reported [743-745].
4.9.2. Classification
Table 7: Classification system for female urethral diverticula based on characteristics*
Localisation | Mid-urethral Distal Proximal Full length |
Configuration | Single Multi-loculated Saddle shaped |
Communication | Mid-urethral No communication visualised Distal Proximal |
Continence | Stress urinary incontinence Continent Post-void dribble Mixed incontinence |
*Limited LNS C3 classification of urethral diverticula .[742,746,747]
4.9.3. Diagnostic evaluation
The commonly encountered symptoms for urethral diverticulum such as pain, urgency, frequency, recurrent UTIs, vaginal discharge, dyspareunia, voiding difficulties or UI [748], are common to many other LUT dysfunctions. Consequently, there is no pathognomonic cluster of symptoms to identify urethral diverticulum. Many patients with urethral diverticulum are asymptomatic. However, urethral diverticulum often presents with a palpable urethral mass. It may be possible to express a purulent exudate from the urethra. Occasionally a stone may develop within the diverticulum.
Urethral diverticulum can be diagnosed by physical examination, VCUG and MRI. Other investigations include urethrocystoscopy, endocavitary (often transvaginal or sometimes transurethral) pelvic floor US and double balloon urethrography.
No robust diagnostic accuracy studies have addressed the question of the best test to confirm the diagnosis in women with clinical suspicion of urethral diverticulum. A case series of 27 patients concluded that endoluminal (vaginal or rectal) MRI has better diagnostic accuracy than VCUG [749] and determines the size and extent of urethral diverticulum more accurately. A case series of 60 patients reported that the sensitivity, specificity, positive predictive value and negative predictive value of MRI was 100%, 83%, 92% and 100%, respectively [750]. Another case series reported 100% specificity and sensitivity of MRI in 60 patients [751]. However, a case series of 41 patients reported a 25% discrepancy between MRI and surgical findings [752]. Endoluminal MRI with either a vaginal or rectal coil may provide even better image quality than simple MRI [753].
Magnetic resonance imaging is the gold standard for the diagnosis and planning of surgical repair and is also useful in diagnosing diverticular inflammation or tumour [754,755].
Urethrocystoscopy can be used to visualise the ostia of the diverticula. Knowledge of the ostias’ location and number can assist with surgical planning since they need to be closed after diverticulectomy. However, given the challenges of urethroscopy in women, the ostia are only seen in 42% of cases [748].
If VCUG is performed, antero-posterior and lateral images are required to optimally characterise the configuration of the diverticulum. There is a high risk of false negatives since the ostia of the diverticula must be patent and the patients must be able to void during the study. In more complex diverticula where there is septation, the entire diverticulum may not be visualised underestimating its complexity or size [756]. The sensitivity of VCUG is 73.5% which is significantly worse than MRI [748].
Ultrasound can be performed transabdominally, trans-vaginally or trans-perineally to identify the diverticulum. In particular, the transvaginal approach allows imaging of the urethra from the meatus to the bladder neck in several planes and can identify the number, size, location, and contents of the diverticulum. This technique is challenging and requires a skilled ultrasonographer. Additionally, the probe can compress the urethra, causing distortion [756]. A meta-analysis reported that US of any kind had a sensitivity of 82.0%, which was inferior to that of MRI [756]. However, a recent publication on trans-labial US reported a sensitivity of 95% [757]; therefore, this approach may be explored further by researchers in the future.
For patients who cannot undergo MRI and those in whom the ostia cannot be seen on cystoscopy, double balloon urethrography is an option. Sensitivity of 94.7% has been reported, which is comparable to that of MRI, but it is technically difficult, requires an experienced radiologist/radiographer and specialised equipment, can be painful for the patient and carries a risk of UTI. Given the current popularity of other imaging modalities, many units may not have access to this technique [756].
4.9.3.1. Associated voiding dysfunction
Although the presentation of urethral diverticulum is often non-specific and variable, urethral diverticulum can be associated with voiding dysfunction and SUI or UUI.
One recent series reported SUI in 60% of patients with urethral diverticulum [758]. Urethral diverticulum is most often located at the level of the mid-urethra. This location often overlaps with the external sphincter. However, urethral diverticulum may also extend proximally toward the bladder neck in the vicinity of the proximal sphincter mechanism. This morphology may, in part, explain the association between urethral diverticulum and SUI, with potentially more proximal lesions at risk for postoperative SUI [759].
Urethral diverticulum may also be associated with BOO due to the mass effect of the urethral diverticulum, urinary retention, or urgency and UUI [760]. Pain and dysuria associated with urethral diverticulum may also result in acquired voiding dysfunction.
Pressure–flow studies may have a role in the preoperative assessment of patients with urethral diverticula and coexisting voiding dysfunction or SUI [741,761-763]. Indeed, urodynamics may evaluate coexisting detrusor dysfunction or document the presence of SUI or obstruction prior to repair [764,765].
Urethral pressure profilometry has also been used in the assessment or diagnosis of urethral diverticulum, noting a biphasic pattern, or pressure drop at the level of the lesion [761,763,766]. Video-urodynamics may be helpful in differentiating SUI from paradoxical UI due to fluid accumulation in the urethral diverticulum. Additionally, resting and straining images obtained during fluoroscopic imaging may document an open bladder neck at rest. This may be a consideration in some patients with an extensive urethral diverticulum at the level of the mid-urethra, and potential implications for postoperative UI due to compromise of both sphincter mechanisms.
4.9.4. Disease management
For women with minimal symptoms who would prefer to avoid invasive treatment, conservative management can be considered. Patients should be warned of the small risk of cancer (1–6%) within the diverticulum [767,768].
4.9.4.1. Surgical treatment
No RCTs have investigated the effectiveness of surgery in women who have a bothersome urethral diverticulum. Thorough evaluation of the anatomy of the diverticulum is essential in planning reconstructive surgery.
There are three surgical approaches to treatment of diverticulum: marsupialisation, endoscopic incision, and curative treatment with diverticulectomy.
Surgical removal (diverticulectomy) is the most commonly reported treatment in contemporary case series. The principles of successful transvaginal diverticulectomy are to: dissect a well-vascularised vaginal flap; preserve the peri-urethral fascia for closure; remove all the diverticular wall; excise the ostium and close the urethra in a watertight fashion; close the incision in a multi-layered fashion with no overlapping suture lines; and preservation or creation of continence.
The decision to use a labial fat pad flap (commonly known as a Martius flap) varies, and the flap is used more frequently in the following situations: recurrent cases, large urethral defects or for deficient vaginal flaps for closure [742,746] transection of the urethra required for access to a circumferential diverticulum [755] or in the case of complex configuration [760], and if there is a planned future sling procedure required for UI to facilitate the dissection at that time [742].
Marsupialisation involves incision into the mass on the vaginal side to drain the infected contents. The wall is sutured open with absorbable suture to allow drainage and prevent reaccumulating of infectious materials. This approach leaves the cystic structure in place and can theoretically cause a urethro-vaginal fistula because there is communication with the diverticular ostium, but it is a rapid procedure with little dissection required. This approach has been advocated in pregnant patients to decompress the diverticulum and allow safe vaginal delivery. A small case series suggested that 75% of pregnant women with urethral diverticula managed expectantly eventually required postpartum surgery [769].
Endoscopic incision is a rarely reported treatment option [770,771]. This procedure involves finding the narrow neck of the ostium and incising it with a resectoscope. This unroofing of the diverticulum transforms the narrow communication with the urethra that causes symptoms when it becomes obstructed into a wide-mouthed sac that drains freely.
4.9.4.2. Management of concomitant stress urinary incontinence
Many women present with concomitant SUI and urethral diverticulum and may request both conditions to be simultaneously treated. A meta-analysis reported that diverticulectomy cured SUI even without a concomitant anti-incontinence procedure. However, no data regarding symptom severity were given and it could be assumed that many of these cured patients had less-severe UI before surgery [748]. Therefore, additional surgical correction may be required [759,771]. However, there is no consensus on appropriate timing of surgical management of these two conditions. Thus, patients with symptomatic bothersome SUI in association with urethral diverticulum may be offered simultaneous anti-UI surgery. Although historical series have shown good results with concomitant bladder neck suspension [765], more contemporary series have utilised pubovaginal fascial slings, with satisfactory outcomes [772-775]. Synthetic MUS are not recommended as a concomitant anti-UI procedure at the time of urethral diverticulectomy [776]. Synthetic material adjacent to a fresh suture line following diverticulectomy in the setting of potentially infected urine may place the patient at higher risk for subsequent urethral erosion and vaginal extrusion of the sling material, as well as urethro-vaginal fistula formation and foreign body granuloma formation.
4.9.4.3. Success rate and complications
Transvaginal urethral diverticulectomy has a high success rate (defined by being dry) of 84–98%, with a reoperation rate of 2–13% after primary repair during a mean follow-up of twelve to 50 months [739,742,759,777]. The resolution of symptoms after surgery has been reported to reach 68.8% but less than half of studies comment on symptom improvement [778].
One case series reported a recurrence rate of 33% in U-shaped and of 60% in circumferential diverticula within one year [746], one study found a 10.7% recurrence rate in 122 women undergoing diverticulectomy, with a higher risk of recurrence in those with proximal or multiple diverticula or after previous pelvic surgery [779] or radiation. Recurrent urethral diverticulum following initial successful urethral diverticulectomy may occur as a result of a new infection or traumatic insult such as childbirth, a new urethral diverticulum, or recurrence of the original lesion. Recurrence may be due to incomplete removal of the urethral diverticulum, inadequate closure of the urethra, residual dead space (circumferential diverticula), or other technical factors. Repeat urethral diverticulectomy represents a unique challenge due to altered anatomy, scarring, and difficulty identifying proper anatomical planes.
One case series reported that storage symptoms decreased significantly postoperatively from 60% to 16% following surgery for urethral diverticulum [759]. Other series with long-term follow-up, however, have demonstrated rates of postoperative urgency of 54% [779], and de novo UUI in 36% of patients [771]. Such postoperative symptoms indicate persistence of urethral diverticulum, recurrence of urethral diverticulum, or de novo OAB syndrome or urethral obstruction.
Stress urinary incontinence can be worsened or occur de novo after diverticulectomy. This is most likely due to sphincteric damage from the dissection or scarification preventing urethral closure. De novo SUI (10.6% of women) seems to be more common in proximal and large (> 30 mm) diverticula [759]. However, a retrospective review noted at least some de novo SUI in 49% of patients following urethral diverticulectomy; most of which was minor and did not require additional therapy [780]. Only 10% of these individuals underwent subsequent SUI surgery. Treatment for SUI after diverticulectomy is not well described in the literature. The most commonly reported operation is an autologous pubovaginal sling [770] followed by retropubic suspension [771]. However, there are two reported cases of synthetic mesh sling to treat SUI, without mesh complications [746,759], but this is controversial.
Early common postoperative complications include UTI (0–39%), de novo SUI (3.8–33%), and de novo urinary retention (0–9%), especially in the setting of concomitant placement of an autologous pubovaginal sling [739,742,759,777]. Delayed complications such as urethral stricture are reported in 0–5.2% of cases [739,742,771,777]. Urethro-vaginal fistula is a devastating complication presenting in 0.9–8.3% of cases [781]. A distal fistula located beyond the sphincteric mechanism can present with split urinary stream or vaginal voiding and may not require repair. However, a fistula located anywhere from the mid-urethra to the bladder neck may result in UI. These patients should undergo repair with consideration of an adjuvant tissue flap, such as a Martius flap, to aid in closure. The timing of the fistula repair is not well defined, with a delay of three to six months after the initial repair being a good balance between patient discomfort and optimal tissue quality. Rare complications include: distal urethral necrosis, bladder injury, urethral injury, ureteric injury, and vaginal scarring or narrowing with consequent dyspareunia [781].
4.9.4.4. Pathological findings
Most urethral diverticula are lined with squamous cells, urothelium or columnar epithelium [742,782,783]. In a meta-analysis, there was a high prevalence of chronic or acute inflammation (68.6%) and the most commonly reported lesions were nephrogenic metaplasia, which occurred in 8% of cases. Diverticula may undergo neoplastic alterations (6%), including invasive adenocarcinoma [784], followed by squamous cell carcinoma in 0.7%. It is unknown if the diverticulum forms first and then transforms into a malignancy or if the malignancy develops first. These malignancies are treated in a similar fashion to urethral cancer in women.
4.9.5. Summary of evidence and recommendations for urethral diverticulum
Summary of evidence | LE |
Magnetic resonance imaging has the best sensitivity and specificity for the diagnosis of urethral diverticulum. | 3 |
Surgical removal of symptomatic urethral diverticulum provides good long-term results; however, women should be counselled of the risk of recurrence and de novo SUI. | 3 |
Recommendations | Strength rating |
Use magnetic resonance imaging for diagnosis and characterisation of urethral diverticula, with urethroscopy, voiding cystourethrogram and ultrasound where necessary. | Weak |
Offer surgical removal of symptomatic urethral diverticulum. | Weak |
If conservative treatment is adopted, warn patients of the small (1–6%) risk of cancer developing within the diverticulum. | Weak |
Carefully question and investigate patients for coexisting voiding dysfunction and urinary incontinence (UI). | Strong |
Following appropriate counselling, address bothersome stress urinary incontinence at the time of urethral diverticulectomy with concomitant non-synthetic sling. | Weak |
Counsel patients regarding the possibility of de novo or persistent LUTS including UI, despite technically successful urethral diverticulectomy. | Strong |