Results of ESUO section surveys spark discussion of what should be considered office urology
Exploring office urology in Europe is an important goal of the EAU Section of Urologists in Office (ESUO).
Exploring office urology in Europe is an important goal of the EAU Section of Urologists in Office (ESUO). It was founded nearly three years ago to represent and promote the interests of office urologists in Europe beyond national structures. The designation ‘office’ seemed to be appropriate to characterise the difference between office urologists’ field of work, that is mainly treating outpatients, and clinical urologists’ field of work, the treatment of inpatients. Key characteristics of office urologists were thought to be “self-employment” and the “privately conducted office”. However, as we have learned, and as you’ll see below, these properties may not be comprehensive enough to address all the urologists who are predominantly treating outpatients.
Investigating the essence of office urologists’ work in the European countries is one core task of the ESUO section - besides conducting educational meetings at EAU meetings and invited lectures at national congresses. Therefore, we made a survey two years ago that explored the number of office urologists and the diagnostic and therapeutic methods office urologists used. The results were published in European Urology Today, issue October/December 2018, p. 23, and the EUT Congress News, 18 March 2019.
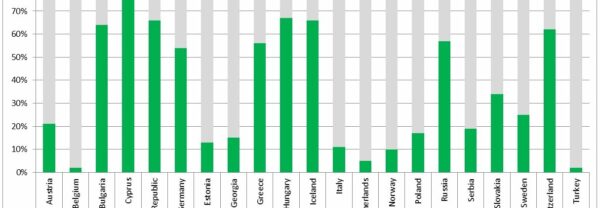
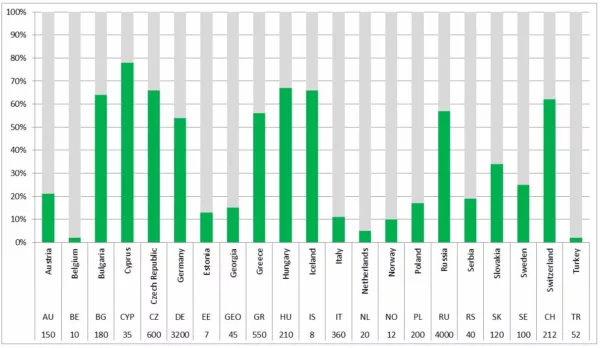
Afterward, we received information from more countries. We learned that there are more than 10,000 office urologists in Europe (fig. 1). The percentage share of office urologists in the individual countries ranges from 2% to 78%. The average share of office urologists in all responding countries is 38%. This surprisingly high proportion is explained by the large absolute number of office urologists in Russia and Germany. But our knowledge is still incomplete, because we lack information from several countries, as can be deduced from the white spots on our map.
Recently, we have conducted a second survey, this time about the working conditions and the working environment of office urologists in different European countries. This survey was done through a questionnaire in September 2019. Section members in 11 countries* who considered themselves to be office urologists reported the numbers. These numbers are estimations, because many official databases used different criteria. So, the figures don’t claim to be representative, but they give a strong impression of the diversity of outpatient urology in European countries.
The results are remarkable - also for us - and make us think about a re-definition of what we consider to be office urology. Plus, they encourage us to cross boundaries in our comprehension of office and outpatient urology, because we see that this field in urology probably has a much wider range than we imagined.
The results of the surveys Approvals:
The health care sector is mostly under the control of state authorities. In work areas where the urologist is not alone in deciding what to do, one or more institutions must approve. These authorities are public and private health care institutions, medical self-administration and government administration. Local hospitals or local urologists may influence the urologist’s decision only in the fields of outpatient surgery, inpatient treatment and – occasionally – medical devices.
Starting an office:
65% of the office urologists in the replying countries are allowed to start offices at any location they want. 10% need the approval of health insurance organisations, 20% of their medical administration, and 25% of government authorities.
Methods and equipment (fig. 2):
Oncological treatment is in most of the countries controlled by official institutions. From our first survey, we know that in nearly all countries oncological drug treatment can be carried out in office; at least treatment of prostate cancer with classical ADT (LHRH and anti-androgens). In half of the countries, therapy using enzalutamide, abiraterone, and instillation therapy for bladder cancer is given in office as well. The in-office use of new substances in renal cancer or chemotherapy is solely allowed in a few countries (e.g. Germany) through a special individual qualification. On the other hand, office urologists are extensively free in administering other drug treatments. The use of certain medical equipment (e.g. ultrasound) has to be approved in only a few countries. In Poland, urologists need no approval at all if they have passed the FEBU exam.
Patients:
On average, 50% (range: 10% - 100%) of the patients visit the office urologist by their own decision. 30% (range: 10% - 60%) are referred by their general practitioners, 15% (range: 10% - 25%) by other specialists. In 5% mentioned other reasons unknown.
Medical associations:
In only 2 countries, Italy and Sweden, associations have been established which are fully dedicated to office or private urologists exclusively. In about 50% of the responding countries, we find local networks of office urologists, some of them collaborating with general practitioners.
Salaries of office urologists:
Nearly 50% (range: 15% - 100%) of the office urologists’ income comes from public, another 18% (range: 5% - 100%) from private health insurances. 28% (1% - 95%) is covered by the patient her/himself, and 5% by hospitals.
The employment of office urologists:
Our data show that in 40% of the countries the office urologists work self-employed in own offices, another 10% are employed in private medical centres. 40% are employed by and based in a hospital. 10% work as part-time employees in a hospital, but have an own office as well and work there during more than half of their working time.
Figure 2: Who/which institution has to decide/agree which methods you may use in your office? Multiple answers were possible.
Uncertainties in defining “office urology”
When we started our ESUO project three years ago, we had the impression (maybe influenced by our home countries) that “self-employment” and “privately conducted office” were the core characteristics of office urologists. By now, we have learned that office urology has a significant larger spectrum. Not only because of office urology’s wide range between office-only urologists on the one hand and office urologists regularly treating inpatients on the other, including flowing transitions and differences from country to country, but also with respect to the kind of their employment and the institutions they work at. Our recent survey shows that only in one half of the countries office urologists work in privately conducted offices (self-employed) or medical centres (employed). The same proportion is employed in hospitals, with some of them running a private office self-employed in addition. For instance, in some countries, office urologists are hospital-based but self-employed. Moreover, colleagues from other countries have told us that some urologists do the same labour as office urologists hospital-based, but refuse this designation and demand the name “outpatient clinic” to characterize their institution. In summary, we see that what we simply call “office urology” is in reality, country-dependent, a different and complex structure of institutions, employment, payment, and patient-and- specialties relations. Also, we have to consider that we might exclude urologists from other countries from our section because of the word "office".
A prudent course of action would now be to extend our target group through a redefinition of office urology to ensure that we include all urologists in this EAU section who fulfil the same tasks as (we thought ‘only’) office urologists do. This could boil down to European urologists who treat outpatients in their main profession in more than 50% of their working time within the context of an established professional profile no matter whether they are office- or hospital-based, who do so not only temporarily, and who are part of an institutionalised link between general medicine and clinical inpatient urology.
What about the future?
Some countries tell us that changes in the hospital and office landscape will lead to changes in the patients’ care. When full departments (of urology) in small hospitals are shut and relocated into those of larger clinics they often are substituted by medical outpatient centres to ensure the nearer-to-home care of outpatients. Private practices are increasingly being bought up by supra-regional commercial enterprises and operated with employed urologists.
These are new challenges for the office and outpatient urology.
The discussion is open! Please send an email to esuo@uroweb.org.
*) Georgia, Germany, Greece, Italy, the Netherlands, Poland, Russia, Serbia, Sweden, Switzerland, United Kingdom