7. DISEASE MANAGEMENT
7.1. Counselling of smoking cessation
It has been confirmed that smoking increases the risk of tumour recurrence and progression in NMIBC patients [239,240] (LE: 3). While it is still controversial whether smoking cessation in BC will favourably influence the outcome of BC treatment, patients should be counselled to stop smoking due to the general health risks associated with tobacco smoking [229,241-243] (LE: 3).
7.2. Office-based fulguration and laser vaporisation
In patients with a history of small Ta LG/G1 tumours, fulguration, or laser vaporisation of small papillary recurrences on an outpatient basis can reduce the therapeutic burden [244,245] (LE: 3). In a prospective RCT, laser photocoagulation with intravesical lidocaine in an outpatient setting proved non inferior to standard TURB under general anaesthesia for the 4 months recurrence rate. Notably, the laser fulguration procedure resulted in only a modest pain score (2.4) and was preferred by 98% of patients [246] (LE: 1b).
7.3. Active Surveillance
With recurrence in LG(G1)Ta tumours being more likely low grade and non-invasive [247-249] the risk of progression to a higher grade or stage is infrequent to rare [250-252]. Expectant management or active surveillance (AS), offer an alternative to TURB and office-based fulguration. Observing no progression to MIBC, Soloway et al., first recommended this approach in 2003 [253] and Miyake et al., subsequently proposed an algorithm for AS using changes in size and multifocality as triggers for intervention [254]. However, from a review undertaken by the EAU Young Academic Urology group [255], it appears that the level of evidence in favour of AS is low, with observational studies having heterogenous selection criteria, triggers for intervention and surveillance tools. The multicentre prospective Bladder Cancer Italian Active Surveillance (BIAS) project, conversely, demonstrated that AS is feasible in selected patients [256,257]; however, additional evidence from quality clinical trials is required.
7.4. Adjuvant intravesical treatment
Although TURB by itself can eradicate a TaT1 tumour completely, these tumours commonly recur and can progress to MIBC. The high variability in the 3-month recurrence rate indicates that the TURB was incomplete or provokes recurrences in a high percentage of patients [151]. It is therefore necessary to consider adjuvant therapy in all patients.
7.4.1. Post-operative irrigation
Two systematic reviews [258,259] and one meta-analysis [260] suggest efficacy of continuous irrigation in the prevention of early recurrences. In case intravesical chemotherapy is not feasible, irrigation of the bladder might be considered.
7.4.2. Intravesical chemotherapy
7.4.2.1. A single, immediate, post-operative intravesical instillation of chemotherapy
Immediate single instillation (SI) has been shown to act by destroying circulating tumour cells after TURB, and by an ablative effect on residual tumour cells at the resection site and on small overlooked tumours [261-264] (LE: 3).
Four large meta-analyses comprising 1,476 to 3,103 patients have consistently shown that after TURB, SI significantly reduces the recurrence rate compared to TURB alone [265-268] (LE: 1a). In a systematic review and individual patient data meta-analysis of 2,278 eligible patients [265], SI reduced the 5-year recurrence rate by 14%, from 59% to 45%. Only patients with primary tumours or intermediate-risk recurrent tumours with a prior recurrence rate of < 1 recurrence/year and those with a 2006 EORTC recurrence score < 5 benefited from SI. In patients with a 2006 EORTC recurrence score > 5 and/or patients with a prior recurrence rate of > 1 recurrence per year, SI was not effective as a single adjuvant treatment. No randomised comparisons of individual drugs have been conducted [265-268].
Single instillation with mitomycin C (MMC), epirubicin or pirarubicin [265], as well as gemcitabine [268], have all shown to lower the intravesical recurrence rate. Single instillation with gemcitabine was superior to saline in a RCT with approximately 200 patients per arm with remarkably low toxicity rates [269]. These findings are in contrast with a previous study, which, however, used a shorter instillation time [270]. In the Böhle et al., study, continuous saline irrigation was used for 24 hours post-operatively in both arms, which could explain the low recurrence rate in the control arm [270].
Prevention of tumour cell implantation should be initiated within the first few hours after TURB. After that, tumour cells are firmly implanted and are covered by the extracellular matrix [261,271-273] (LE: 3). In all SI studies, the instillation was administered within 24 hours. Two RCTs found no overall impact of SI with apaziquone; in contrast, a post-hoc analysis did find a reduction of recurrence risk in patients receiving apaziquone within
90 minutes following TURB [274].
To maximise the efficacy of SI, one should devise flexible practices that allow the instillation to be given as soon as possible after TURB, preferably within the first two hours in the recovery room or even in the operating theatre. As severe complications have been reported in patients with drug extravasation, safety measures should be maintained (see Section 7.7) [275,276]. To allow for optimal compliance with this Level 1 evidence, clinical teams are encouraged to explore barriers and facilitators within their practice [277].
7.4.2.2. Additional adjuvant intravesical chemotherapy instillations
The need for further adjuvant intravesical therapy depends on prognosis. In low-risk patients (Tables 6.1 and 6.2), a SI reduces the risk of recurrence and is considered to be the standard and complete treatment [265,266] (LE: 1a). For other patients, however, a SI remains an incomplete treatment because of the considerable likelihood of recurrence and/or progression (Tables 6.1 and 6.2). Efficacy data for the following comparisons of application schemes were published.
Single installation only vs. SI and further repeat instillations
In one study, further chemotherapy instillations after SI improved RFS in intermediate-risk patients [278] (LE: 2a).
Repeat chemotherapy instillations vs. no adjuvant treatment
A large meta-analysis of 3,703 patients from 11 RCTs showed a highly significant (44%) reduction in the odds of recurrence at one year in favour of chemotherapy over TURB alone [279]. This corresponds to an absolute difference of 13–14% in the proportion of patients with recurrence. Contrary to these findings, two meta-analyses have demonstrated that BCG therapy may also reduce the risk of tumour progression [280,281] (see Section 7.2.2.1) (LE: 1a). Moreover, BCG maintenance therapy appears to be significantly better in preventing recurrences than chemotherapy [282-284] (see Section 7.2.2.1) (LE: 1a). However, BCG causes significantly more side effects than chemotherapy [284] (LE: 1a).
Single instillation + further repeat instillations vs. later repeat instillations only
There is evidence from several studies in intermediate-risk patients that SI might have an impact on recurrence even when further adjuvant instillations are given [285-288]. A RCT including 2,243 NMIBC patients, which compared SI of MMC with an instillation of MMC delayed two weeks after TURB (followed by further repeat instillations in both treatment arms), showed a significant reduction of 9% in the risk of recurrence at 3 years in favour of SI, from 36% to 27%. The effect was significant in the intermediate- and high-risk groups of patients receiving additional adjuvant MMC instillations [285] (LE: 2a). Since the author’s definition of the risk groups differed significantly in the initial publication, they adapted their patient stratification in the second analysis and consistently showed improved efficacy of SI followed by repeat MMC instillations [289]. The results of this study should be considered with caution since some patients did not receive adequate therapy. Another RCT found no impact of SI with epirubicin followed by further chemotherapy or BCG instillations in a cohort of predominant HR BC patients [290].
The optimal schedule of intravesical chemotherapy instillations
The length and frequency of repeat chemotherapy instillations is still controversial; however, it should not exceed one year [288] (LE: 3).
7.4.2.3. Options for improving efficacy of intravesical chemotherapy
7.4.2.3.1. Adjustment of pH, duration of instillation, and drug concentration
Two prospective RCTs showed that optimized intravesical administration of MMC reduced recurrence rates, either by a combination of measures (higher MMC-dose, peroral sodium bicarbonate, and refraining from drinking) [291] and by adding cytosine arabinoside [292], respectively (LE: 1b). The value of these measures in addition to alternative maintenance schedules is not known. Another trial reported that duration of a one-hour instillation of MMC was more effective compared to a 30-minute instillation, but no efficacy comparisons are available for one- vs. two-hour durations of instillation [293] (LE: 3). Another RCT using epirubicin has documented that concentration is more important than treatment duration [294] (LE: 1b). In view of these data, instructions are provided (see Section 7.7).
7.4.2.3.2. Device-assisted intravesical chemotherapy
Hyperthermic intravesical chemotherapy
Different technologies which increase the temperature of instilled MMC are available. A recent systematic review and meta-analysis including 4 RCTs suggests similar toxicity as for BCG with maintenance schedule [295].
Microwave-induced hyperthermia effect (RITE)
Promising data have been presented on enhancing the efficacy of MMC using microwave-induced hyperthermia in patients with high-risk tumours [296]. In one RCT comparing one year of BCG with one year MMC and microwave-induced hyperthermia in patients with intermediate- and high-risk BC, increased RFS at 24 months in the MMC group was demonstrated [297] (LE: 1b).
Conductive chemohyperthermia
In an open-label phase II RCT including 259 patients, HIVEC chemo-hyperthermia failed to demonstrate an improvement in DFS at 24 months over standard adjuvant intravesical chemotherapy in intermediate-risk NMIBC (61% vs. 60%), with a higher risk of treatment discontinuation (59% vs. 89% of completed planned treatments) [298].
In a pilot phase II RCT on 50 high-risk NMIBCs, HIVEC™ MMC showed early outcomes comparable to BCG (24 months RFS, 86.5% with HIVEC™ and 71.8% with BCG, p = 0.184) [299]. These data needs to be corroborated by further studies.
Electromotive drug administration
The efficacy of MMC using electromotive drug administration (EMDA) sequentially combined with BCG in patients with high-risk tumours has been demonstrated in one small RCT [300]. The definitive conclusion, however, needs further confirmation. For application of device-assisted instillations in patients recurring after BCG treatment, see Section 7.9.3.
7.4.2.4. Summary of evidence - intravesical chemotherapy
Summary of evidence | LE |
In patients with low-risk NMIBC and in those with a small Ta LG/G1 recurrence detected more than one year after previous TURB, a SI significantly reduces the recurrence rate compared to TURB alone. | 1a |
Single instillation might have an impact on recurrence even when further adjuvant chemotherapy instillations are given. | 3 |
Repeat chemotherapy instillations (with or without previous SI) improve RFS in intermediate-risk patients. | 2a |
7.4.3. Intravesical bacillus Calmette-Guérin (BCG) immunotherapy
7.4.3.1. Efficacy of BCG
7.4.3.1.1. Recurrence rate
Five meta-analyses have confirmed that BCG after TURB is superior to TURB alone or TURB plus chemotherapy for preventing the recurrence of NMIBC [282,301-304] (LE: 1a). Three RCTs of intermediate- and high-risk tumours have compared BCG with epirubicin and interferon (INF) [305], MMC [306], or epirubicin alone [283] and have confirmed the superiority of BCG for prevention of tumour recurrence (LE: 1a). The effect is long lasting [283,306] and was also observed in a separate analysis of patients with intermediate-risk tumours [283]. One meta-analysis [282] has evaluated the individual data from 2,820 patients enrolled in 9 RCTs that have compared MMC vs. BCG. In the trials with BCG maintenance, there was a 32% reduction in the risk of recurrence for BCG compared to MMC, but a 28% increase in the risk of recurrence for patients treated with BCG in the trials without BCG maintenance. A Cochrane systematic review confirmed that BCG is more effective in reducing the recurrence rate over MMC [307].
7.4.3.1.2. Progression rate
Two meta-analyses have demonstrated that BCG therapy delays and potentially lowers the risk of tumour progression [280,281,304] (LE: 1a). A meta-analysis carried out by the EORTC GUCG has evaluated data from 4,863 patients enrolled in 24 RCTs. In 20 of the trials, some form of BCG maintenance was used. Based on a median follow-up of 2.5 years, tumours progressed in 9.8% of the patients treated with BCG compared to 13.8% in the control groups (TURB alone, TURB and intravesical chemotherapy, or TURB with the addition of other immunotherapy). This shows a reduction of 27% in the odds of progression with BCG maintenance treatment. The size of the reduction was similar in patients with TaT1 papillary tumours and in those with CIS [281]. A RCT with long-term follow-up has demonstrated significantly fewer distant metastases and better overall- and disease-specific survival in patients treated with BCG compared to epirubicin [283] (LE: 1b). In contrast, an individual patient data meta-analysis and Cochrane review were not able to confirm any statistically significant difference between MMC and BCG for progression, survival, and cause of death [282,307].
The conflicting results in the outcomes of these studies can be explained by different patient characteristics, duration of follow-up, methodology and statistical power. However, most studies showed a reduction in the risk of progression in high-and intermediate-risk tumours if a BCG maintenance schedule was applied.
7.4.3.1.3. Influence of further factors
Two other meta-analyses have suggested a possible bias in favour of BCG arising from the inclusion of patients previously treated with intravesical chemotherapy [308]. In the individual patient data meta-analysis, however, BCG maintenance was more effective than MMC in reduction of recurrence rate, both in patients previously treated and not previously treated with chemotherapy [282] (LE: 1a). It was demonstrated that BCG was less effective in patients > 70 years of age, but still more effective than epirubicin in a cohort of elderly patients [309] (LE: 1a). According to a cohort analysis, the risk of tumour recurrence after BCG was shown to be higher in patients with a previous history of UTUC [310].
7.4.3.2. BCG strain
Although smaller studies without maintenance demonstrated some differences between strains [310-312], a network meta-analysis identified ten different BCG strains used for intravesical treatment in the published literature but was not able to confirm superiority of any BCG strain over another [313].
Similarly, a published meta-analysis of prospective RCTs [281], published data from a prospective registry [314] as well as from a post-hoc analysis of a large phase II prospective trial assessing BCG and INF-α in both BCG-naive and BCG-failure patients did not suggest any clear difference in efficacy between the different BCG strains [315] (LE: 2a). The quality of data, however, does not allow definitive conclusions.
7.4.3.3. BCG toxicity
Bacillus Calmette-Guérin intravesical treatment is associated with more side effects compared to intravesical chemotherapy [281,307] (LE: 1a). However, serious side effects are encountered in < 5% of patients and can be treated effectively in almost all cases [316] (LE: 1b). The incidence of BCG infections after BCG instillations was 1% in a registry-based cohort analysis [317]. It has been shown that a maintenance schedule is not associated with an increased risk of side effects compared to an induction course [316]. Side effects requiring treatment stoppage were seen more often in the first year of therapy [318]. Elderly patients do not seem to experience more side effects leading to treatment discontinuation [319] (LE: 2a). No significant difference in toxicity between different BCG strains was demonstrated [314]. Symptoms may be the result of side effects of the BCG treatment or caused by bladder disease (widespread CIS) itself. Consequently, the burden of symptoms is reduced after completion of the treatment in a significant number of patients [320].
Major complications can appear after systemic absorption of the drug. Thus, contraindications of BCG intravesical instillation should be respected (see Section 7.9). The presence of leukocyturia, nonvisible haematuria or asymptomatic bacteriuria is not a contraindication for BCG application, and antibiotic prophylaxis is not necessary in these cases [121,321] (LE: 3). Three RCTs suggest reduced side effects by administering different quinolones in conjunction with the BCG-instillations [322-324]. The latter, by using two doses of levofloxacin in conjunction with each BCG-instillation, reduced the proportion of patients with high-grade side effects, both local (pollakisuria) and systemic (fever), and additionally displayed improved PFS in the experimental arm [324] (LE: 1b).
Bacillus Calmette-Guérin should be used with caution in immunocompromised patients; e.g., immunosuppression, human immunodeficiency virus (HIV) infection poses relative contraindications [325], although some small studies have shown similar efficacy and no increase in complications compared to non-immunocompromised patients. The role of prophylactic anti-tuberculosis medication in these patients remains unclear [326-328] (LE: 3). The management of side effects after BCG should reflect their type and grade according to the recommendations provided by the International Bladder Cancer Group (IBCG) and by a Spanish group [329,330] (Table 7.1).
Table 7.1: Management options for side effects associated with intravesical BCG [330-333]
Management options for local side effects (modified from International Bladder Cancer Group) | |
Symptoms of cystitis | Phenazopyridine, propantheline bromide, or non-steroidal anti-inflammatory drugs (NSAIDs). |
If symptoms improve within a few days: continue instillations. | |
If symptoms persist or worsen: | |
If symptoms persist even with antibiotic treatment: a.With positive culture: adjust antibiotic treatment according to sensitivity b.With negative culture: quinolones and potentially analgesic anti-inflammatory instillations once daily for 5 days (repeat cycle if necessary) [331]. | |
If symptoms persist: anti-tuberculosis drugs + corticosteroids. | |
If no response to treatment and/or contracted bladder: radical cystectomy. | |
Haematuria | Perform urine culture to exclude haemorrhagic cystitis if other symptoms present. |
If haematuria persists, perform cystoscopy to evaluate presence of bladder tumour. | |
Symptomatic granulomatous prostatitis | Symptoms rarely present: perform urine culture. |
Quinolones. | |
If quinolones are not effective: isoniazid (300 mg/day) and rifampicin (600 mg/day) for 3 months. | |
Cessation of intravesical therapy. | |
Epididymo-orchitis [332] | Perform urine culture and administer quinolones. |
Cessation of intravesical therapy. | |
Orchidectomy if abscess or no response to treatment. | |
Management options for systemic side effects | |
General malaise, fever | Generally resolve within 48 hours, with or without antipyretics. |
Arthralgia and/or arthritis | Rare complication and considered autoimmune reaction. |
Arthralgia: treatment with NSAIDs. | |
Reactive arthritis: NSAIDs. | |
If no/partial response, proceed to corticosteroids, high-dose quinolones or antituberculosis drugs [333]. | |
Persistent high-grade fever (> 38.5°C for > 48 h) | Permanent discontinuation of BCG instillations. |
Immediate evaluation: urine culture, blood tests, chest X-ray. | |
Prompt treatment with more than two antimicrobial agents while diagnostic evaluation is conducted. | |
Consultation with an infectious diseases specialist. | |
BCG sepsis | Prevention: initiate BCG at least 2 weeks post-transurethral resection of the bladder (if no signs and symptoms of haematuria). |
Cessation of BCG. | |
For severe infection: High-dose quinolones or isoniazid, rifampicin, and ethambutol 1.2 g daily for Early, high-dose corticosteroids as long as symptoms persist. Consider an empirical non-specific antibiotic to cover Gram-negative bacteria and/or Enterococcus. | |
Allergic reactions | Antihistamines and anti-inflammatory agents. |
Consider high-dose quinolones or isoniazid and rifampicin for persistent symptoms. | |
Delay therapy until reactions resolve. | |
* Persistent severe cystitis symptoms associated with BCG use have a high risk to underlie a complicated UTI (even in the absence of a positive culture) and thus no restriction applies to the empirical use of quinolones by the Pharmacovigilance Risk Assessment Committee of the EMA (see also Section 3.7 Complicated UTI and 3.7.4.1- Choice of antimicrobials of the EAU Guidelines on Urological Infection 2022) [7].
7.4.3.4. Optimal BCG schedule
Induction BCG instillations are given according to the empirical 6-weekly schedule introduced by Morales et al., [335]. For optimal efficacy, BCG must be given in a maintenance schedule [280-282,304] (LE: 1a). Many different maintenance schedules have been used, ranging from a total of 10 instillations given in 18 to 27 weeks over 3 years [336].
7.4.3.4.1. Optimal number of induction instillations and frequency of instillations during maintenance
The optimal number of induction instillations and frequency of maintenance instillations were evaluated by NIMBUS, a prospective phase III RCT. Safety analysis after 345 randomised patients demonstrated that a reduced number of instillations (3 instillations in induction and 2 instillations at 3, 6 and 12 months) proved inferior to the standard schedule (6 instillation in induction and 3 instillations at 3, 6 and 12 months) regarding the time to first recurrence [337] (LE: 1b). In a RCT including 397 patients CUETO showed that in high-risk tumours a maintenance schedule with only one instillation every 3 months for 3 years was not superior to induction therapy only, which suggested that one instillation may be suboptimal to 3 instillations in each maintenance cycle [338] (LE: 1b).
7.4.3.4.2. Optimal length of maintenance
In their meta-analysis, Böhle et al., concluded that at least one year of maintenance BCG is required to obtain superiority of BCG over MMC for prevention of recurrence or progression [280] (LE: 1a).
In a RCT of 1,355 patients, the EORTC has shown that when BCG is given at full dose, 3 years’ maintenance (3-weekly instillations 3, 6, 12, 18, 24, 30 and 36 months) reduces the recurrence rate compared to one year in high- but not in intermediate-risk patients. There were no differences in progression or OS. In the 3-year arm, however, 36.1% of patients did not complete the 3-year schedule [339] (LE: 1b). The main reason why these patients stopped treatment was treatment inefficacy, not toxicity.
7.4.3.5. Optimal dose of BCG
To reduce BCG toxicity, instillation of a reduced dose was proposed. However, it has been suggested that a full dose of BCG is more effective in multifocal tumours [340,341] (LE: 1b). The CUETO study compared one-third dose to full-dose BCG and found no overall difference in efficacy. One-third of the standard dose of BCG might be the minimum effective dose for intermediate-risk tumours. A further reduction to one-sixth dose resulted in a decrease in efficacy with no decrease in toxicity [342] (LE: 1b). The EORTC did not find any difference in toxicity between one-third and full-dose BCG, but one-third dose BCG was associated with a higher recurrence rate, especially when it was given only for one year [318,339] (LE: 1b). In a recent meta-analysis of 9 RCTs, patients who received less than half of the standard BCG dose experienced less adverse events as compared to patients receiving the full dose, but suffered more recurrences [343].
7.4.3.6. BCG shortage
A statement by the Panel on BCG shortage can be accessed online: https://uroweb.org/guidelines/non-muscle-invasive-bladder-cancer/publications-appendices.
7.4.3.7. Summary of evidence - BCG treatment
Summary of evidence | LE |
In patients with intermediate- and high-risk tumours, intravesical BCG after TURB reduces the risk of tumour recurrence; it is more effective than TURB alone or TURB and intravesical chemotherapy. | 1a |
For optimal efficacy, BCG must be given in a maintenance schedule. | 1a |
Three-year maintenance is more effective than one year to prevent recurrence in patients with high-risk tumours, but not in patients with intermediate-risk tumours. | 1a |
7.4.4. Combination therapy
7.4.4.1. Intravesical BCG plus chemotherapy versus BCG alone
In one RCT, a combination of MMC and BCG was shown to be more effective in reducing the risk of disease recurrence while increasing toxicity compared to BCG monotherapy (LE: 1b). Using similar BCG schedules in both groups, each BCG instillation in the combination group was preceded a day before by an added MMC instillation [344]. In a RCT using MMC with EMDA, a combination of BCG and MMC with EMDA showed an improved recurrence-free interval and reduced progression rate compared to BCG monotherapy [300,345] (LE: 2). Two meta-analyses demonstrated improved disease-free survival (DFS), but no benefit in PFS in patients treated with combination treatment comparing to BCG monotherapy [345,346].
7.4.4.2. Combination treatment using interferon
In a Cochrane meta-analysis of 4 RCTs, a combination of BCG and IFN-2α did not show a clear difference in recurrence and progression over BCG alone [347]. In one study, weekly MMC followed by monthly BCG alternating with IFN-2α showed a higher probability of recurrence compared to MMC followed by BCG alone [348]. Additionally, a RCT in a similar population of NMIBC comparing BCG monotherapy with a combination of epirubicin and INF for up to two years showed the latter was significantly inferior to BCG monotherapy in preventing recurrence [349] (LE: 1b).
7.4.4.3. Sequential chemotherapy instillations
Preclinical data suggest that the efficacy of intravesical chemotherapy instillations can be improved by combinations compared to the administration of single agents only [350]. Sequential (immediate) instillations of gemcitabine and docetaxel was initially reported in 2015 in the wake of BCG-shortage but also at times of limited access to mitomycin [351]. Subsequently other sequential chemotherapy combinations such as valrubicin and docetaxel have been suggested [352]. Over time, additional retrospective data have accumulated where sequential gemcitabine and docetaxel instillations were used in patients recurring after induction BCG and BCG-unresponsive disease [353]; in patients with recurrence after BCG-induction but not fulfilling the criteria for BCG-unresponsive disease [354]; and also in BCG-naïve high-risk patients [355]. Thus, in patients with BCG-unresponsive disease when the treatment standard (radical cystectomy) is not feasible due to age and/or comorbidity or when patients are unwilling to accept radical surgery, sequential instillations with gemcitabine and docetaxel is an emerging treatment concept awaiting further prospective scientific evaluation.
7.4.5. Specific aspects of treatment of carcinoma in situ
7.4.5.1. Treatment strategy
The detection of concurrent CIS increases the risk of recurrence and progression of TaT1 tumours [222,224]. In this case further treatment according to the criteria summarised in Sections 7.4.2, 7.4.3 and 7.9 is mandatory. Carcinoma in situ cannot be cured by an endoscopic procedure alone. Histological diagnosis of CIS must be followed by further treatment, either intravesical BCG instillations or RC (LE: 4). Tumour-specific survival rates after immediate RC for CIS are excellent, but a large proportion of patients might be over-treated [232] (LE: 3).
7.4.5.2. Cohort studies on intravesical BCG or chemotherapy
In retrospective evaluations of patients with CIS, a complete response rate of 48% was achieved with intravesical chemotherapy and 72−93% with BCG [232-235,356] (LE: 2a). Up to 50% of complete responders might eventually show recurrence with a risk of invasion and/or extravesical recurrence [235,273,336,356] (LE: 3).
7.4.5.3. Prospective randomised trials on intravesical BCG or chemotherapy
Unfortunately, there have been few RCTs in patients with CIS only. A meta-analysis of clinical trials comparing intravesical BCG to intravesical chemotherapy in patients with CIS has shown a significantly increased response rate after BCG and a reduction of 59% in the odds of treatment failure with BCG [357] (LE: 1a).
In an EORTC-GUCG meta-analysis of tumour progression, in a subgroup of 403 patients with CIS, BCG reduced the risk of progression by 35% as compared to intravesical chemotherapy or immunotherapy [281] (LE: 1b). The combination of BCG and MMC was not superior to BCG alone [358]. In summary, compared to chemotherapy, BCG treatment of CIS increases the complete response rate, the overall percentage of patients who remain disease free, and reduces the risk of tumour progression (LE: 1b).
7.4.5.4. Treatment of CIS in the prostatic urethra and upper urinary tract
Patients with CIS are at high risk of extravesical involvement in the UUT and in the prostatic urethra. Solsona et al., found that 63% of 138 patients with CIS developed extravesical involvement initially or during follow-up [359]. Patients with extravesical involvement had worse survival than those with bladder CIS alone [359] (LE: 3). In the prostate, CIS might be present only in the epithelial lining of the prostatic urethra or in the prostatic ducts [360]. These situations should be distinguished from tumour invasion into the prostatic stroma (stage T4a in bladder tumours) and for which immediate radical cystoprostatectomy is mandatory. Patients with CIS in the epithelial lining of the prostatic urethra can be treated by intravesical instillation of BCG. Transurethral resection of the prostate can improve contact of BCG with the prostatic urethra [146,361] (LE: 3). However, potential spread of CIS has to be considered; no suprapubic trocar-placed catheter should be used.
In patients with prostatic duct involvement there are promising results of BCG, but only from small series. The data are insufficient to provide clear treatment recommendations and radical surgery should be considered [361,362] (LE: 3).
7.4.5.5. Summary of evidence - treatment of carcinoma in situ
Summary of evidence | LE |
Carcinoma in situ cannot be cured by an endoscopic procedure alone. | 4 |
Compared to intravesical chemotherapy, intravesical BCG maintenance instillations increase the complete response rate, the overall percentage of patients who remain disease free, and reduce the risk of tumour progression. | 1b |
7.5. Intravesical chemoablation and neoadjuvant treatment
Older marker lesion studies have shown that chemoablation with a single intravesical chemotherapy instillation can achieve a complete response in a proportion of patients [363]. In addition, hypothesis-generating findings from an older RCT comparing immediate pre-operative device-assisted (EMDA) MMC with post-operative SI with MMC and TURB only, showed improved long-term RFS among patients treated prior to TURB [364], and thus even suggest a long-term effect after neoadjuvant instillations. While this has not been reproduced by other groups, additional neoadjuvant clinical trials were recently published. In recurrent low-risk [365] and recurrent Ta tumours [366], 4 and 6 intravesical MMC instillations achieved complete response in 37% and 57% of the patients, respectively. The former study prematurely stopped recruitment as the anticipated 45% complete response after chemoablation was not achieved. Compared to TURB, less dysuria and incontinence occurred in the intervention arm of the trial. Before routine clinical application, additional high-level evidence with RFS as an outcome measure is required.
7.6. Radical cystectomy for non-muscle-invasive bladder cancer
There are several reasons to consider immediate RC for selected patients with NMIBC:
- The staging accuracy for T1 tumours by TURB is low with 27–51% of patients being upstaged to muscle-invasive tumour at RC [182,367-371] (LE: 3).
- Some patients with NMIBC experience disease progression to muscle-invasive disease (Table 6.2).
- Patients who experience disease progression to muscle-invasive stage have a worse prognosis than those who present with ‘primary’ muscle-invasive disease [372,373].
The potential benefit of RC must be weighed against its risks, morbidity, and impact on quality of life (QoL) and discussed with patients, in a shared decision-making process. It is reasonable to propose immediate RC in those patients with NMIBC who are at very high risk of disease progression (see Section 6.3 and Tables 6.1 and 6.2) [75,179,222,224,374] (LE: 3).
Early RC is strongly recommended in patients with BCG-unresponsive tumours and should be considered in BCG relapsing HG tumours as mentioned in Section 7.9 and Table 7.3. A delay in RC may lead to decreased disease-specific survival [375] (LE: 3).
In patients in whom RC is performed before progression to MIBC, the 5-year DFS rate exceeds 80% [376-378] (LE: 3).
7.7. Primary treatment by disease type
The type of further therapy after TURB should be based on the risk groups shown in Section 6.3 and Table 6.1. The stratification and treatment recommendations are based on the risk of disease progression. In particular in intermediate-risk tumours, the 2006 EORTC scoring model may be used (Section 6.1.1.1) to determine a patient’s individual risk of disease recurrence as the basis to decide further treatment on.
- Treatment of low-risk disease
Patients in the low-risk group have a negligible risk of disease progression. The single post-operative instillation of chemotherapy reduces the risk of recurrence and is considered as sufficient treatment in these patients.
- Treatment of intermediate-risk disease
Patients in the intermediate-risk group have a low risk of disease progression (7.4 and 8.5% after 10 years according to the 2021 EAU NMIBC scoring model). In these patients one-year full-dose BCG treatment (induction plus 3-weekly instillations at 3, 6 and 12 months), or instillations of chemotherapy (the optimal schedule is not known) for a maximum of one year, is recommended. The final choice should reflect the individual patient’s risk of recurrence and progression as well as the efficacy and side effects of each treatment modality.
- Treatment of high-risk disease
Patients in the high-risk group have a high risk of disease progression (14.1 and 14.2% after 10 years according to the 2021 EAU NMIBC scoring model). In these patients full-dose intravesical BCG for one to 3 years (induction plus 3-weekly instillations at 3, 6, 12, 18, 24, 30 and 36 months), is indicated. The additional beneficial effect of the second and third years of maintenance should be weighed against its added costs, side effects and problems associated with BCG shortage. Because of the high risk of progression, immediate RC may also be discussed with the patient. Radical cystectomy is the safest approach from an oncological point of view, it is, however, associated with the risk of complications and QoL impairment and represents over-treatment in some patients.
- Treatment of very high-risk disease
Patients in the very high-risk group have an extremely high risk of tumour progression (53.1 and 58.6% after 10 years according to the 2021 EAU NMIBC scoring model). Immediate RC should be discussed with these patients. In case RC is not feasible or refused by the patient, full-dose intravesical BCG for one to 3 years should be offered.
- Treatment of carcinoma in situ
Patients with carcinoma in situ cannot be managed by an endoscopic procedure alone and should be offered either intravesical BCG instillations or RC (LE: 4). BCG treatment of CIS increases the complete response rate, the overall percentage of patients who remain disease free, and reduces the risk of tumour progression (LE: 1b). In comparison, immediate RC for CIS results in excellent tumour-specific survival rates although a large proportion of patients might be over-treated [232] (LE: 3).
7.8. Multidisciplinary tumour board
A multidisciplinary tumour board (MDT) approach including reassessment of radiology and pathology is associated with a changed treatment plan in up to 44% of BC patients [379], such as refraining from or recommending cystectomy in 7% of stage T1 patients [380-382], often as a result of the pathologic review [70,381]. Thus, patients with high-risk and very high-risk NMIBC will especially benefit from MDT discussion and such an approach is recommended for these patients.
Figure 7.1 presents a treatment flow chart based on risk category, which may guide management of an individual patient.
Figure 7.1: Treatment strategy in primary or recurrent tumour(s) without previous BCG*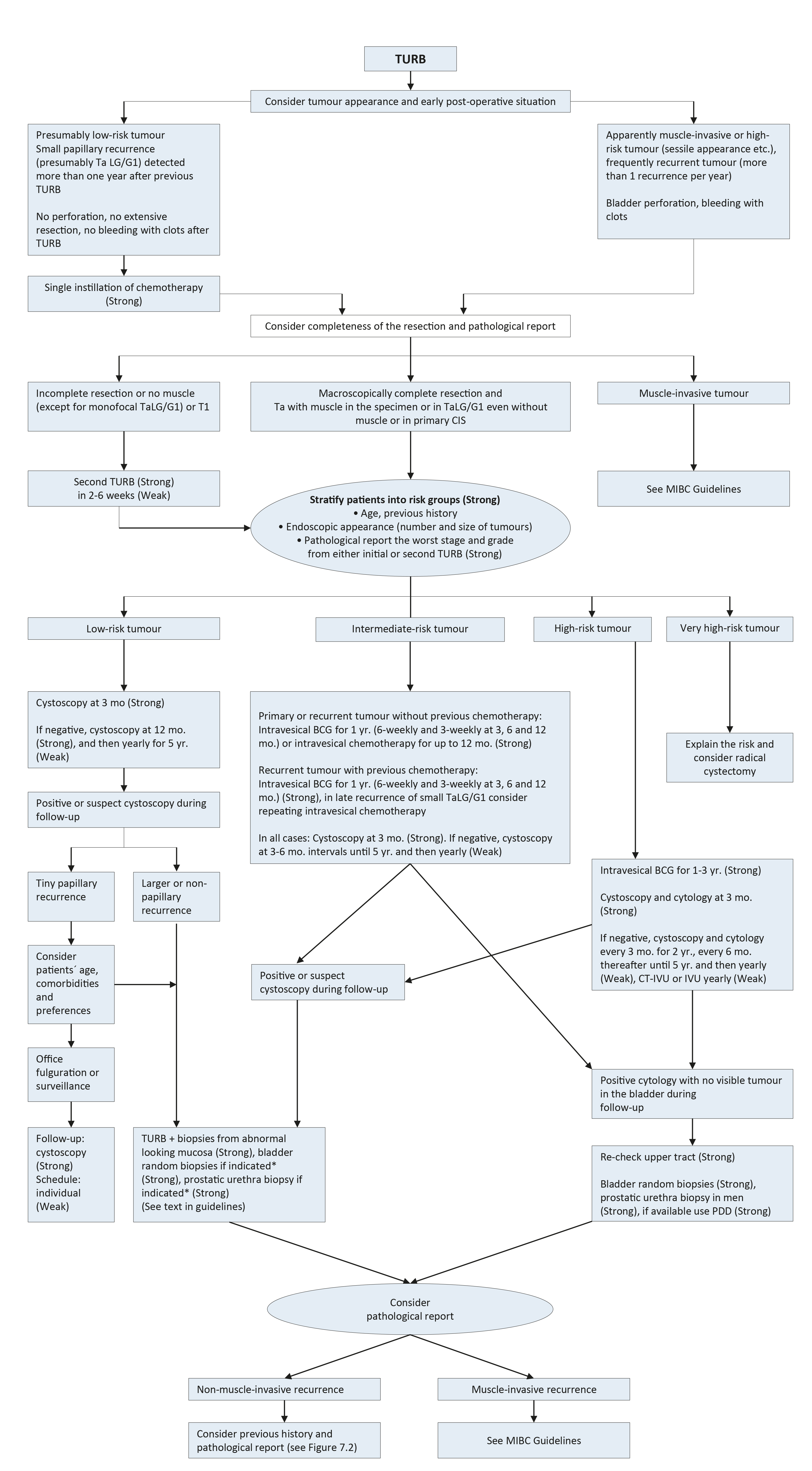 * For details and explanations see the text of the guidelines.
* For details and explanations see the text of the guidelines.
BCG = bacillus Calmette-Guérin; CIS = carcinoma in situ; CT = computed tomography; IVU = intravenous urography; MIBC = muscle-invasive bladder cancer; PDD = photodynamic diagnosis; TURB = transurethral resection of the bladder.
7.9. Treatment of failure of intravesical therapy
7.9.1. Recurrence during or after intravesical chemotherapy
Patients with NMIBC recurrence during or after a chemotherapy regimen can benefit from BCG instillations. Prior intravesical chemotherapy has no impact on the effect of BCG instillations [282] (LE: 1a).
7.9.2. Treatment failure after intravesical BCG immunotherapy
Several categories of BCG failures, broadly defined as any HG disease occurring during or after BCG therapy, have been proposed (see Table 7.2). Non-muscle-invasive BC may not respond at all (BCG refractory) or may relapse after initial response (BCG relapsing). Some evidence suggests that patients with BCG relapse have better outcomes than BCG refractory patients [383].
To be able to specify the subgroup of patients where additional BCG is unlikely to provide benefit, the category of BCG-unresponsive tumour was defined. Further BCG instillations in these patients are associated with an increased risk of progression [236,384]. The category of BCG-unresponsive tumours comprises BCG-refractory and some of BCG-relapsing tumours (see Table 7.2) [385]. The definition was developed in consultation with the U.S. Food and Drug Administration (FDA), in particular to promote single-arm trials to provide primary evidence of effectiveness in this setting [386]. Non-HG recurrence after BCG is not considered as BCG failure.
Table 7.2: Categories of high-grade recurrence during or after BCG
Categories of high-grade recurrence during or after BCG |
Whenever a MIBC is detected during follow-up. |
BCG-refractory tumour |
1. If T1 HG/G3 tumour is present at 3 months [236,384,387] (LE: 3). 2. If Ta HG/G3 tumour is present after 3 months and/or at 6 months, after either re-induction or first course of maintenance [360] (LE: 4). 3. If CIS (without concomitant papillary tumour) is present at 3 months and persists at 6 months after either re-induction or first course of maintenance. If patients with CIS present at 3 months, an additional BCG course can achieve a complete response in > 50% of cases [67,356,360] (LE: 1b). 4. If HG tumour appears during BCG maintenance therapy*. |
BCG-relapsing tumour |
Recurrence of HG/G3) tumour after completion of BCG maintenance, despite an initial response [388] (LE: 3). |
BCG-unresponsive tumour |
BCG-unresponsive tumours include all BCG refractory tumours and those who develop T1/Ta HG recurrence within 6 months of completion of adequate BCG exposure** or develop CIS within 12 months of completion of adequate BCG exposure [385] (LE: 4). |
BCG intolerance |
Severe side effects that prevent further BCG instillation before completing treatment [330]. |
* Patients with LG recurrence during or after BCG treatment are not considered to be a BCG failure.
** Adequate BCG is defined as the completion of at least 5 of 6 doses of an initial induction course plus at least 2 out of 6 doses of a second induction course or 2 out of 3 doses of maintenance therapy.
7.9.3. Treatment of BCG-unresponsive tumours, late BCG-relapsing tumours, LG recurrences after BCG treatment and patients with BCG intolerance
Patients with BCG-unresponsive disease are unlikely to respond to further BCG therapy; RC is therefore the standard and preferred option. Currently, several bladder preservation strategies are being investigated such as cytotoxic intravesical therapies [389-392], device assisted instillations [393-395], intravesical immunotherapy [396,397], systemic immunotherapy [398] or gene therapy [399-401].
A phase III RCT including predominantly high-risk NMIBC patients failing at least a previous induction course of BCG, MMC combined with microwave-induced hyperthermia provided 35% overall DFS at 2 years as compared to 41% in the control arm (treated with either BCG, MMC or MMC and electromotive drug administration at the discretion of the investigator). In the pre-planned sub-analysis, MMC and microwave-induced thermotherapy showed lower response rates in CIS recurrences but higher DFS in non-CIS papillary tumours (53% vs. 24%) [395].
Promising data on BCG-unresponsive cohorts of patients with CIS alone or concomitant to papillary tumours were recently reported following new immunotherapies. Systemic pembrolizumab achieved a 40% complete response rate in a prospective phase II study which was maintained in 48% of patients for up to 12 months (n = 101), resulting in FDA approval of the study drug for this patient population [402]. Promising data from a phase III multicentre RCT with intravesical nadofaragene firadenovec showed a complete response in 53.4% of patients with BCG-unresponsive CIS [403]. A secondary analysis indicates that a combination of post-treatment titres of serum anti–human adenovirus type-5 antibody and fold change from baseline can predict treatment efficacy [404].
A systematic review and meta-analysis including 4 RCTs and 24 single-arm studies (all currently available prospective studies) assessed bladder-sparing treatments following BCG failure [405]. The significant heterogeneity of both trial designs and patient characteristics included in these studies, the different definitions of BCG failures used, and missing information on prior BCG courses may account for the variability in efficacy for the different compounds assessed across different trials. A higher number of previous BCG courses, BCG refractory/unresponsive or CIS predicted lower response rates. The pooled 12-month response rates were 24% for trials with > 2 prior BCG courses and 36% for those with > 1 BCG courses. Initial response rate did not predict durable responses highlighting the need for longer-term follow-up. More recently, a systematic review assessing 42 prospective trials on bladder-preserving treatments after BCG showed that patients with papillary-only recurrences appeared more effectively treated (median recurrence free rate of 44% at 1 year, median progression-free rate of 89% at a median follow-up of 19 months) than CIS-containing tumours (median complete response rate of 17% at 1 year with a median progression-free rate of 95% at a median follow-up of 12 months), highlighting potential biological differences between these two tumour entities which should be analysed separately when reporting results of clinical trials [406].
At the present time, treatments other than RC are considered oncologically inferior in patients with BCG-unresponsive disease [236,384,387] (LE: 3). Various studies suggest that repeat-BCG therapy is appropriate for non-HG and even for some HG recurrent tumours; namely those relapsing beyond one year after BCG exposure (cases which do not meet the criteria of BCG-unresponsive disease) [407,408] (LE: 3).
Treatment decisions in LG recurrences after BCG (which are not considered as any category of BCG failure) should be individualised according to tumour characteristics. Little is known about the optimal treatment in patients with high-risk tumours who could not complete BCG instillations because of intolerance.
7.9.4. Summary of evidence - treatment failure of intravesical therapy
Summary of evidence | LE |
Prior intravesical chemotherapy has no impact on the effect of BCG instillation. | 1a |
Treatments other than RC must be considered oncologically inferior in patients with BCG-unresponsive tumours. | 3 |
Figure 7.2: Treatment strategy in recurrence during or after intravesical BCG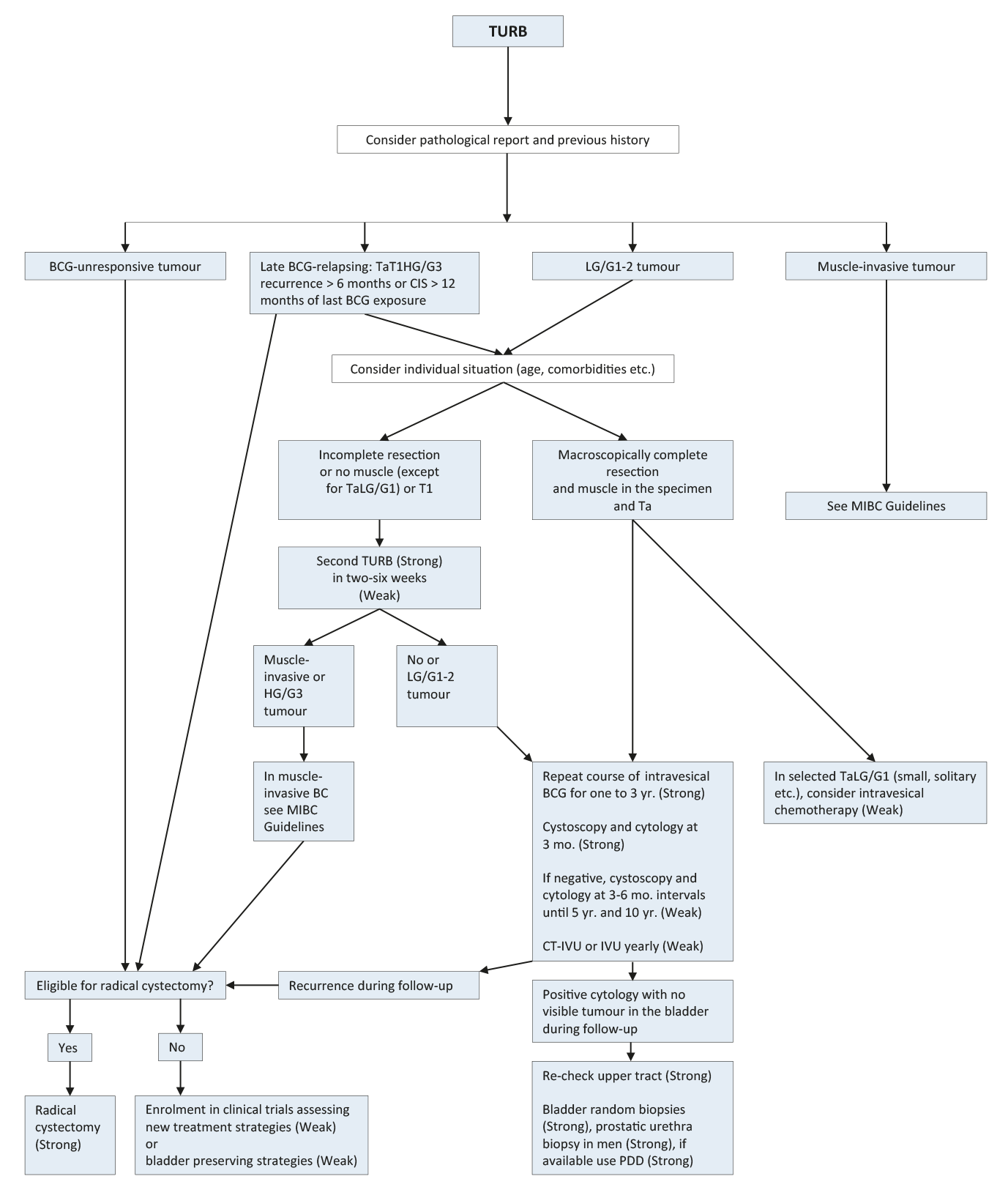 BCG = bacillus Calmette-Guérin; CIS = carcinoma in situ; HG = high-grade; IVU = intravenous urography;LG = low-grade; PDD = photodynamic diagnosis; TURB = transurethral resection of the bladder.
BCG = bacillus Calmette-Guérin; CIS = carcinoma in situ; HG = high-grade; IVU = intravenous urography;LG = low-grade; PDD = photodynamic diagnosis; TURB = transurethral resection of the bladder.
7.10. Guidelines for adjuvant therapy in TaT1 tumours and for therapy of carcinoma in situ
General recommendations | Strength rating |
Counsel smokers to stop smoking. | Strong |
The type of further therapy after transurethral resection of the bladder (TURB) should be based on the risk groups shown in Section 6.3 and Table 6.1. For determination of a patient’s risk group use the 2021 EAU risk group calculator available at www.nmibc.net. | Strong |
In patients with tumours presumed to be at low risk and in those with small papillary recurrences (presumably Ta LG/G1) detected more than one year after previous TURB, offer one immediate single chemotherapy instillation. | Strong |
Offer post-operative saline or water continuous irrigation of the bladder to patients who cannot receive a single instillation of chemotherapy. | Strong |
Patients with small recurrent low-grade Ta tumours can be effectively and safely offered office fulguration. | Strong |
Only offer active surveillance to selected patients with presumed low-risk tumours not amendable to endoscopic ablation. | Weak |
In patients with intermediate-risk tumours (with or without immediate instillation), offer one-year full-dose Bacillus Calmette-Guérin (BCG) treatment (induction plus 3-weekly instillations at 3, 6 and 12 months), or instillations of chemotherapy (the optimal schedule is not known) for a maximum of one year. The final choice should be made in a shared decision-making process with the patient, reflecting his/her risk of recurrence and progression, as well as the efficacy and side effects of each treatment modality. | Strong |
In patients with high-risk tumours, full-dose intravesical BCG for one to 3 years (induction plus 3-weekly instillations at 3, 6, 12, 18, 24, 30 and 36 months), is indicated. The additional beneficial effect of the second and third years of maintenance should be weighed against its added costs, side effects and access to BCG. Immediate radical cystectomy (RC) may also be discussed with the patient. | Strong |
In patients with very high-risk tumours offer immediate RC. Discuss intravesical full-dose BCG instillations for one to 3 years and discuss clinical trials with those who refuse or are unfit for RC. | Strong |
Offer transurethral resection of the prostate, followed by intravesical instillation of BCG to patients with CIS in the epithelial lining of the prostatic urethra. | Weak |
Cautiously offer quinolones to treat BCG-related side effects*. | Weak |
The definition of ‘BCG-unresponsive’ should be respected as it most precisely defines the patients who are unlikely to respond to further BCG instillations. | Strong |
Offer a RC to patients with BCG-unresponsive tumours. | Strong |
Offer patients with BCG-unresponsive tumours, who are not candidates for RC due to comorbidities, preservation strategies (intravesical chemotherapy, chemotherapy and microwave-induced hyperthermia, electromotive administration of chemotherapy, intravesical- or systemic immunotherapy; preferably within clinical trials). | Weak |
Discuss high-risk and very high-risk patients within a multidisciplinary board, when possible. | Weak |
Recommendations - technical aspects for treatment | |
Intravesical chemotherapy | |
If given, administer a single immediate instillation of chemotherapy within 24 hours after TURB. | Weak |
Omit a single immediate instillation of chemotherapy in any case of overt or suspected bladder perforation or bleeding requiring bladder irrigation. | Strong |
The optimal schedule and duration of further intravesical chemotherapy instillation is not defined; however, it should not exceed one year. | Weak |
If intravesical chemotherapy is given, use the drug at its optimal pH and maintain the concentration of the drug by reducing fluid intake before and during instillation. | Strong |
The length of individual instillation should be a minimum of one, and up to two hours. | Weak |
BCG intravesical immunotherapy | |
Absolute contraindications of BCG intravesical instillation are: during the first two weeks after TURB; in patients with visible haematuria; after traumatic catheterisation; in patients with symptomatic urinary tract infection. | Strong |
*The side-effect profile of quinolones and fluoroquinolones resulted in the adoption of European regulation restricting their use [7].
7.11. Guidelines for the treatment of TaT1 tumours and carcinoma in situ according to risk stratification
Recommendations | Strength rating |
EAU risk group: Low | |
Offer one immediate instillation of intravesical chemotherapy after transurethral resection of the bladder (TURB). | Strong |
EAU Risk Group: Intermediate | |
In all patients either one-year full-dose Bacillus Calmette-Guérin (BCG) treatment (induction plus 3-weekly instillations at 3, 6 and 12 months), or instillations of chemotherapy (the optimal schedule is not known) for a maximum of one year is recommended. The final choice should reflect the individual patient’s risk of recurrence and progression as well as the efficacy and side effects of each treatment modality. Offer one immediate chemotherapy instillation to patients with small papillary recurrences detected more than one year after previous TURB. | Strong |
EAU risk group: High | |
Offer intravesical full-dose BCG instillations for one to 3 years but discuss immediate radical cystectomy (RC). | Strong |
EAU risk group: Very High | |
Offer RC or intravesical full-dose BCG instillations for one to 3 years to those who refuse or are unfit for RC. | Strong |
Table 7.3: Treatment options for the various categories of BCG failure
Category | Treatment options |
BCG-unresponsive | 1. Radical cystectomy (RC). |
2. Enrolment in clinical trials assessing new treatment strategies. | |
3. Bladder-preserving strategies in patients unsuitable or refusing RC. | |
Late BCG relapsing: TaT1 HG recurrence > 6 months or CIS > 12 months of last BCG exposure | 1. Radical cystectomy or repeat BCG course according to a patient’s individual situation. |
2. Bladder-preserving strategies. | |
LG recurrence after BCG for primary intermediate-risk tumour | 1. Repeat BCG or intravesical chemotherapy. |
2. Radical cystectomy. |