10. PRIAPISM
Evidence acquisition and limitations
The Panel conducted systematic reviews on the medical and surgical management of ischaemic and non-ischaemic priapism and a dedicated systematic review on the overall management of priapism related to sickle cell disease (SCD). The results of these systematic reviews are presented below in the guidelines and the limitations of the studies that were assessed are highlighted. Most studies had the same limitations and methodological bias: lack of published protocols, retrospective and usually single-arm design, lack of randomisation and blinding, incomplete outcome data, and selective reporting. Additionally, most studies included small numbers of patients, reported non-standardised patient characteristics, and had short (or even unreported) follow-up times and, in general, they reflected single-unit practices.
The definitions of priapism and outcomes (such as success and related complications) were inconsistent across the literature and few of the trials met the clear definitions that were set by the Panel for use in the systematic reviews. Hence, any attempt to draw clinically meaningful conclusions and offer evidence-based guidance based on systematic assessment of the literature was a challenging task. These limitations highlight the urgent need for clear and commonly accepted definitions of conditions and outcomes that should be used by researchers in the future so that robust evidence can be developed to support relevant guidelines and clinical practice recommendations.
The Panel acknowledged the evidence-related limitations, and in accordance with the EAU Guidelines Office methodology, also took into consideration the benefits/harms balance and the patient ideals, views and preferences prior to finalising the relevant recommendations (for/against, weak/strong).
Priapism is a persistent or prolonged erection in the absence of sexual stimulation that fails to subside. It can be divided into ischaemic, non-ischaemic and stuttering priapism.
10.1. Ischaemic (Low-Flow or Veno-Occlusive) Priapism
10.1.1. Epidemiology, aetiology, pathophysiology and diagnosis
Ischaemic priapism is a persistent erection marked by rigidity of the corpora cavernosa and by little or no cavernous arterial inflow [1555]. It presents as a painful rigid erection that is characterised clinically by absent or reduced intracavernous arterial inflow, although proximally there is a compensated high velocity picture with little flow distally [1556]. Ischaemic priapism is the most common subtype of priapism, accounting for > 95% of all episodes [1555,1557]. In ischaemic priapism, there are time-dependent metabolic alterations within the corpus cavernosum progressively leading to hypoxia, hypercapnia, glucopenia and acidosis [1558,1559].
Ischaemic priapism that lasts beyond 4 hours is similar to a compartment syndrome and characterised by the development of ischaemia within the closed space of the corpora cavernosa, which severely compromises the cavernosal circulation. Emergency medical intervention is required to minimise irreversible consequences, such as smooth muscle necrosis, corporal fibrosis and the development of permanent ED [1560,1561]. The duration of ischaemic priapism represents the most significant predictor for the development of ED. In this context, interventions beyond 48-72 hours of onset may help to relieve the erection and pain, but have little clinical benefit in preventing long-term ED [1562].
Histological analysis of corporal smooth muscle biopsies shows that at 12 hours, there are features of interstitial oedema, progressing to destruction of the sinusoidal endothelium, exposure of the basement membrane and thrombocyte adherence by 24 hours. At 48 hours, thrombi in the sinusoidal spaces and smooth muscle necrosis with fibroblast-like cell transformation are evident [1563]. This implies that by 48 hours there appears to be smooth muscle necrosis and irreversibility of these ischaemic changes. A case-control study comparing corporal biopsies from patients with priapism lasting 48-72 hours with control penile tissues retrieved from autopsies demonstrated a significantly lower percentage of smooth muscle fibres, with an increase in elastic fibres and collagen [1560,1564].
No specific pathophysiological causes of ischaemic priapism can be identified in most cases [1555,1565], although the common aetiological factors include SCD, haematological dyscrasias, neoplastic syndromes, and several pharmacological agents (e.g., intracavernosal PGE1 therapy) (Table 45). Ischaemic priapism may occur (0.4-35%) after intracavernosal injection of erectogenic agents [535,1555,1560,1566,1567]. The risk is higher with papaverine-based combinations [1568], while the risk of priapism is < 1% following prostaglandin E1 injection [1569].
Second-generation antipsychotics (33.8%), other medications (11.3%), and alpha-adrenergic antagonists (8.8%) accounted for the greatest percentage of published drug-induced priapism cases [1570]. Isolated cases of priapism have been described in men who have taken PDE5Is [1555]. A recent study from the FDA Adverse Reporting System Public Dashboard showed that PDE5Is-induced priapism accounted for only 2.9% of drug-induced priapism. However, most of these men also had other risk factors for priapism, and it is unclear whether PDE5Is per se can cause ischaemic priapism [1555,1571]. Since most men who experience priapism following PDE5I treatment have additional risk factors for ischaemic priapism, PDE5Is use is usually not regarded as a risk factor in itself. In terms of haemoglobinopathies, SCD is the most common cause of priapism in childhood, accounting for 63% of cases. It is the primary aetiology in 23% of adult cases [1569], and men with SCD have a lifetime probability of 29-42% of developing ischaemic priapism [1569,1572,1573] (LE: 4).
Mechanisms of SCD-associated priapism may involve derangements of several signalling pathways in the penis, resulting in disinhibited vasorelaxation of the cavernous smooth muscle by NOS and Rho-associated protein kinase (ROCK) signalling, and increased oxidative stress associated with nicotinamide adenine dinucleotide phosphate (NADPH) oxidase-mediated signalling. Excessive adenosine and up-regulation of opiorphins in response to hypoxia reduce PDE5 gene expression and activity and impair NO bioavailability in the penis. Excessive oxidative/nitrosative stress and decreased activity of the RhoA/Rho-kinase contractile pathway further promotes priapism. Contrary to traditional belief, maintenance of physiological testosterone levels does not cause priapism, but rather preserves penile homeostasis and promotes normal erectile function [1574,1575]. Testosterone deficiency is considered a controversial risk factor: it is prevalent in patients with SCD, but recent evidence indicates that it is not a risk factor per se for priapism [1576].
Priapism resulting from metastatic or regional infiltration by tumour is rare and usually reflects an infiltrative process, more often involving the bladder and prostate as the primary cancer sites [1577]. In a recent large retrospective study including 412 men with ischaemic priapism, eleven (3.5%) had malignant priapism, of which seven cases were a consequence of local invasion while the others were secondary to haematological malignancy [1578]. The conventional therapeutic recommendations for pharmacological treatment are unlikely to be effective and all of these men should have MRI of the penis and be offered supportive care and medical intervention for their primary cancer. In selected cases where palliative treatment options fail to control penile pain, a palliative penectomy can be considered.
Partial priapism, or idiopathic partial segmental thrombosis of the corpus cavemosum, is a rare condition. It is often classified as a subtype of priapism limited to a single crura without ischaemia, but rather a thrombus is present within the corpus cavernosum. Its aetiology is unknown, but bicycle riding, trauma, drug use, sexual intercourse, haematological diseases and α-blockers intake have all been associated with partial segmental thrombosis [1579]. The presence of a congenital web within the corpora is also a risk factor [1580].
Table 45: Aetiological factors for the development of priapism
Idiopathic |
- |
Haematological dyscrasias, vascular and other disorders |
|
Infections (toxin-mediated) |
|
Metabolic disorders |
|
Neurogenic disorders |
|
Neoplasms (metastatic or regional infiltration) |
|
Medications |
|
10.1.1.1. Summary of evidence on the epidemiology, aetiology and pathophysiology of ischaemic priapism
Summary of evidence | LE |
Ischaemic priapism is the most common type, accounting for more than 95% of all cases. | 1b |
Ischaemic priapism is identified as idiopathic in most patients, while SCD is the most common cause in childhood. | 1b |
Ischaemic priapism occurs relatively often (about 5%) after intracavernous injections of papaverine-based combinations, while it is rare (< 1%) after prostaglandin E1 monotherapy. | 2a |
Priapism is rare in men who have taken PDE5Is, with only sporadic cases reported. | 4 |
10.1.2. Diagnostic evaluation
10.1.2.1. History
Taking a comprehensive history is critical in priapism diagnosis and treatment [1555,1581]. The medical history must specifically enquire about SCD or any other haematological abnormality [1582,1583] and a history of pelvic, genital or perineal trauma. The sexual history must include the duration of the erection, the presence and degree of pain, prior drug treatment, history of priapism and erectile function prior to the last priapism episode (Table 45). The history can help to determine the underlying priapism subtype (Table 46). Ischaemic priapism is classically associated with progressive penile pain and the erection is rigid. However, non-ischaemic priapism is often painless and the erections often fluctuate in rigidity.
Table 46: Key points in the history for a priapism patient (adapted from Broderick et al. [1555])
Duration of erection |
Presence and severity of pain |
Previous episodes of priapism and methods of treatment |
Current erectile function, especially the use of any erectogenic therapies prescription or nutritional supplements |
Medications and recreational drug use |
Sickle cell disease, haemoglobinopathies, hypercoagulable states, vessel vasculitis |
Trauma to the pelvis, perineum or penis |
10.1.2.2. Physical examination
In ischaemic priapism, the corpora are fully rigid and tender, but the glans penis is soft. The patient complains of severe pain. Pelvic examination may reveal an underlying pelvic or genitourinary malignancy [1578].
10.1.2.3. Laboratory testing
Laboratory testing should include a complete blood count, white blood cell count with blood cell differential, platelet count and coagulation profile to assess anaemia and detect haematological abnormalities [1555,1581].
A genome-wide association study on Brazilian patients identified four single nucleotide polymorphisms in LINC02537 and NAALADL2 significantly associated with priapism, although testing is not routinely recommended in clinical practice [1584].
Aspiration of blood from the corpora cavernosa usually reveals dark ischaemic blood (Table 47) (LE: 2b). Blood gas analysis is essential to differentiate between ischaemic and non-ischaemic priapism (Table 48). Further laboratory testing should be directed by the history, clinical examination and laboratory findings. These may include specific tests (e.g., haemoglobin electrophoresis) for diagnosis of SCD or other haemoglobinopathies.
10.1.2.4. Penile imaging
Colour Doppler US of the penis and perineum is recommended after clinical diagnosis and can differentiate ischaemic from non-ischaemic priapism as an alternative or adjunct to blood gas analysis [1556,1585-1587] (LE: 2b). Colour Doppler US can identify the presence of the fistula as a blush with 100% sensitivity and 73% specificity [1587].
Ultrasound scanning of the penis should be performed before corporal blood aspiration in ischaemic priapism to prevent aberrant blood flow which can mimic a non-ischaemic picture or reperfusion picture after intervention for low-flow priapism [1588].
Following Colour Doppler US there will be an absence of blood flow in the cavernosal arteries in ischaemic priapism. Return of the cavernous artery waveform indicates successful detumescence [1555,1587,1589]. After aspiration, reactive hyperaemia may develop with a high arterial flow proximally that may be misleading and result in the diagnosis of non-ischaemic priapism.
Penile MRI can be used in the diagnostic evaluation of priapism and may be helpful in selected cases of ischaemic priapism to assess the viability of the corpora cavernosa and the presence of penile fibrosis. In particular, in cases of refractory priapism or delayed presentation (> 48 hours), smooth muscle viability can be indirectly assessed. In a prospective study of 38 patients with ischaemic priapism, the sensitivity of MRI in predicting non-viable smooth muscle was 100%, when correlated with corpus cavernosum biopsies [1588]. In this study, all patients with viable smooth muscle on MRI maintained erectile function on clinical follow-up with the non-viable group being offered an early prosthesis.
Table 47: Key findings in priapism (adapted from Broderick et al. [1555])
Ischaemic priapism | Non-ischaemic priapism | |
Corpora cavernosa fully rigid | Typically | Seldom |
Penile pain | Typically | Seldom |
Abnormal penile blood gas | Typically | Seldom |
Haematological abnormalities | Sometimes | Seldom |
Recent intracavernosal injection | Sometimes | Sometimes |
Perineal trauma | Seldom | Typically |
Table 48: Typical blood gas values (adapted from Broderick et al. [1555])
Source | pO2 (mmHg) | pCO2 (mmHg) | pH |
Normal arterial blood (room air) (similar values are found in arterial priapism) | > 90 | < 40 | 7.40 |
Normal mixed venous blood (room air) | 40 | 50 | 7.35 |
Ischaemic priapism (first corporal aspirate) | < 30 | > 60 | < 7.25 |
Figure 13: Differential diagnosis of priapism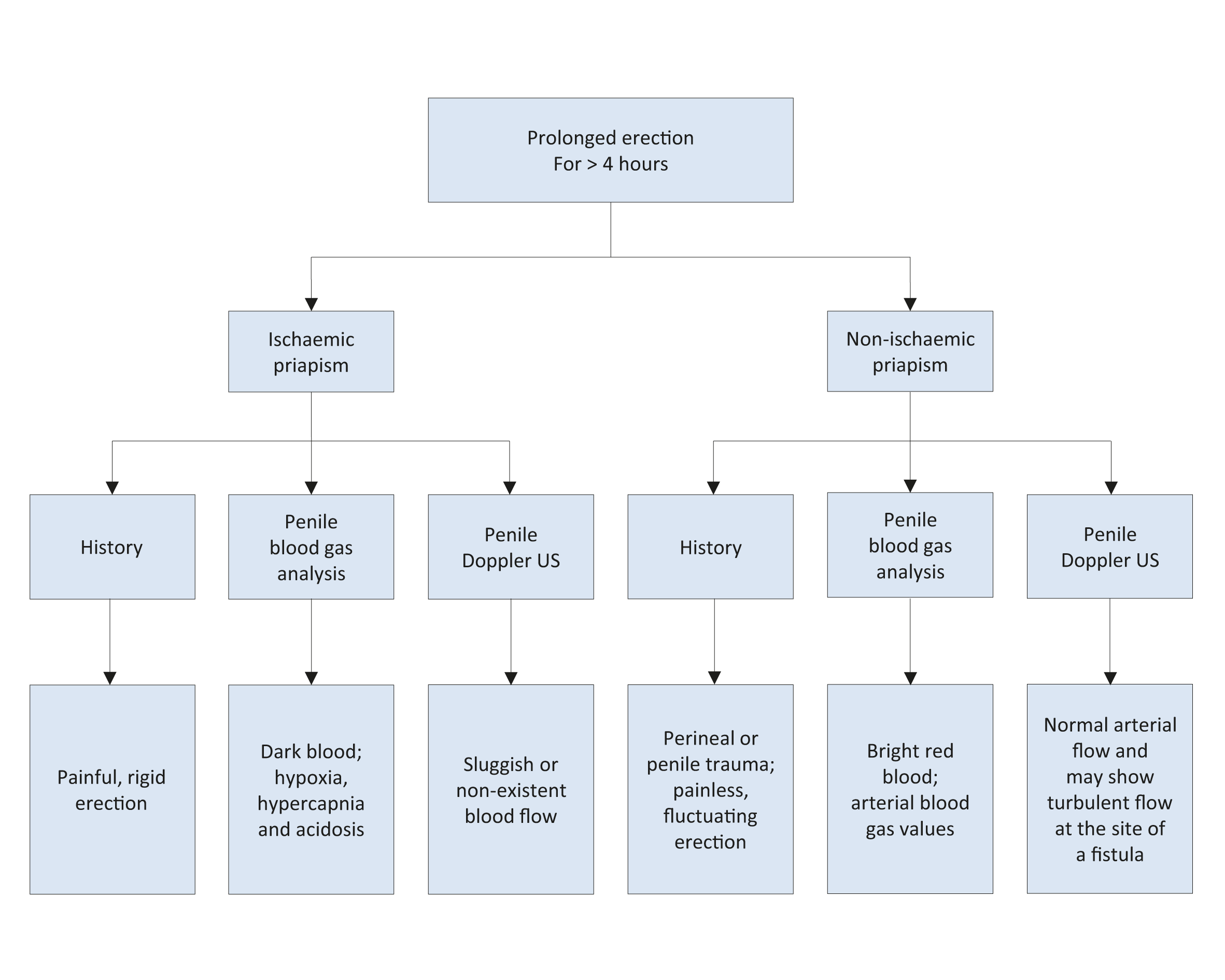
10.1.2.5. Recommendations for the diagnosis of ischaemic priapism
Recommendations | Strength rating |
Take a comprehensive history to establish the diagnosis which can help to determine the priapism subtype. | Strong |
Include a physical examination of the genitalia, perineum and abdomen in the diagnostic evaluation. | Strong |
For laboratory testing, include a full blood count, white blood cell count with blood cell differential, platelet count and coagulation profile. Directed further laboratory testing should be performed depending upon history and clinical and laboratory findings. In children with priapism, perform a complete evaluation of all possible causes. | Strong |
Perform a haemoglobinopathy screen in patients with low flow priapism who are at high risk of sickle cell disease or thalassemia. | Strong |
Analyse the blood gas parameters from blood aspirated from the penis to differentiate between ischaemic and non-ischaemic priapism. | Strong |
Perform colour duplex ultrasound of the penis and perineum before aspiration to differentiate between ischaemic and non-ischaemic priapism. | Strong |
Use magnetic resonance imaging of the penis in cases of prolonged ischaemic priapism or refractory priapism, as an adjunct to predict smooth muscle viability. | Weak |
Perform selected pudendal arteriogram when embolisation is planned for the management of non-ischaemic priapism. | Strong |
Acute ischaemic priapism is a medical emergency. Urgent intervention is mandatory and should follow a stepwise approach. The aim of any treatment is to restore penile detumescence, without pain, in order to prevent corporal smooth muscle fibrosis and subsequent ED.
Figure 14: Medical and surgical management of ischaemic priapism
The treatment is sequential and physicians should move on to the next stage if treatment fails.
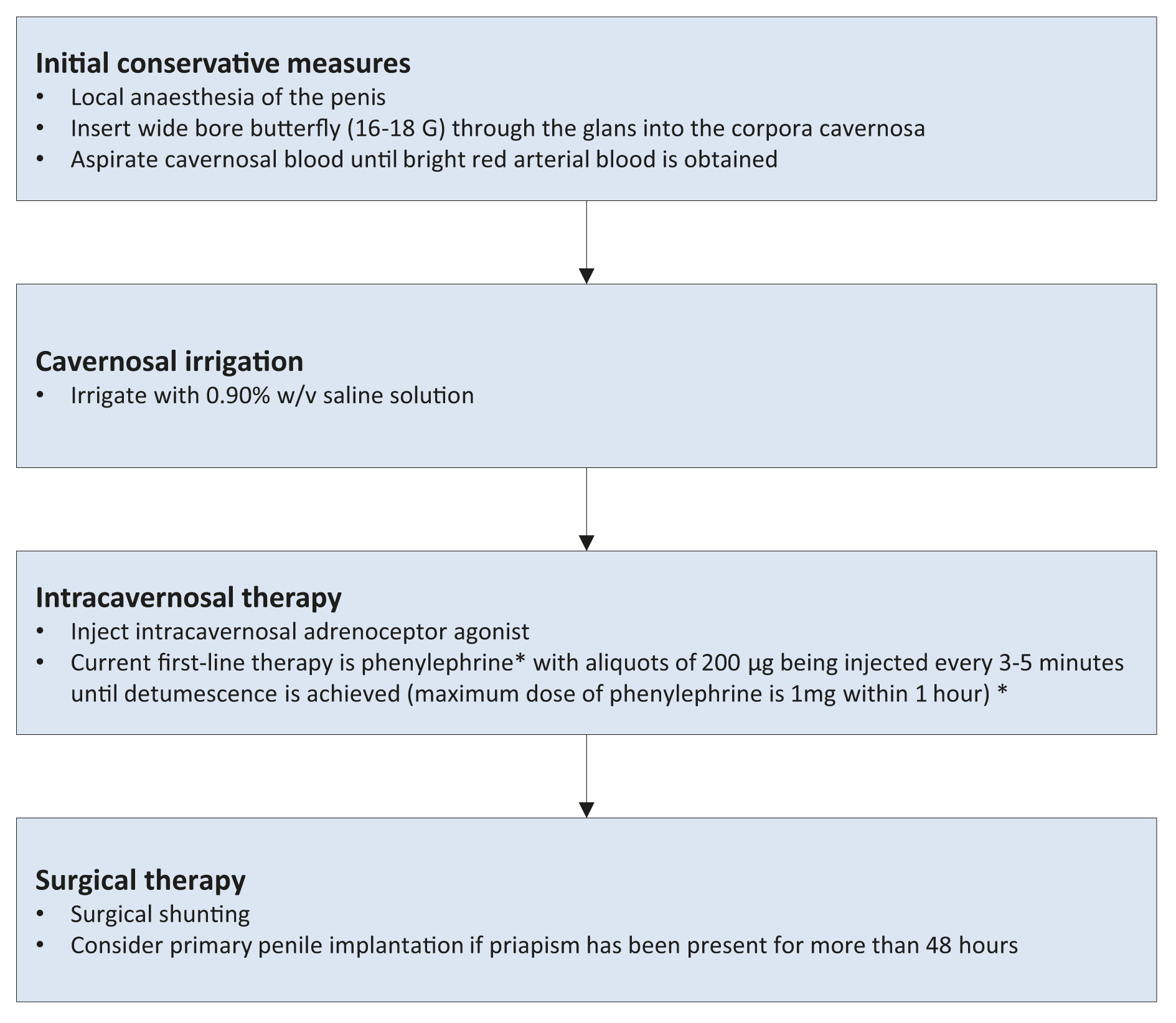 (*) Dose of phenylephrine should be reduced in children. It can result in significant hypertension and shouldbe used with caution in men with cardiovascular disease. Monitoring of pulse and blood pressure is advisable in all patients during administration and for one hour afterwards. Its use is contraindicated in men with a history of cerebro-vascular disease and significant hypertension.
(*) Dose of phenylephrine should be reduced in children. It can result in significant hypertension and shouldbe used with caution in men with cardiovascular disease. Monitoring of pulse and blood pressure is advisable in all patients during administration and for one hour afterwards. Its use is contraindicated in men with a history of cerebro-vascular disease and significant hypertension.
10.1.3. Disease management
10.1.3.1. Medical management
Evidence acquisition
The studies that were identified after abstract screening and used for this literature review pertaining to medical management are reported in the table in Appendix 1 online supplementary evidence. Most of these studies were retrospective case series without an available protocol. Additionally, several limitations were encountered during their assessment, including small study samples, unclear definitions of conditions, interventions and outcomes, short or no reported follow-up and selective reporting of outcomes. As such, providing clinicians with clear recommendations based on robust evidence was not possible. Based on the studies included in the Panel’s systematic review, medical management of priapism demonstrates a wide range of effectiveness, although it seems that sexual dysfunction and complication rates in medical management responders were not high, when reported. It should be emphasised that most patients included in the surgical management studies that are discussed below represent medical non-responders. The selection bias that by definition existed in the surgical management in these single-arm studies makes the estimation of true effectiveness of medical intervention difficult to quantify.
10.1.3.1.1. First-line treatments
First-line medical treatments of ischaemic priapism of more than 4 hours duration are strongly recommended before any surgical treatment (LE: 4). Conversely, first-line treatments initiated beyond 48 hours, while relieving priapism, have little documented benefit in terms of long-term potency preservation (LE: 4). This is likely to be the consequence of irreversible smooth muscle hypoxia and damage that begins to be established by approximately 48 hours of onset of ischaemia [1560-1562]. An in-vitro model of priapism has shown that there is window of opportunity for therapeutic intervention beyond which the recovery of functional erectile tissue is unlikely due to irreversible smooth muscle cell dysfunction [1558]. In line with this finding it has been shown in a series of 50 patients with low-flow priapism who were successfully treated and followed-up for a mean of
66 months, those with priapism lasting for more than 48 hours had a significant risk of ED [1560].
Historically, several first-line treatments have been described including exercise, ejaculation, ice packs, cold baths, and cold water enemas [1555]. However, there is limited evidence for the benefit of such measures and they may even exacerbate crisis in SCD patients. Success rates of these conservative measures alone have been rarely reported. In a small series, for instance, cold water enemas have been reported to induce detumescence in six out of ten cases [1590]. In another study 24.5% of 122 patients achieved detumescence following priapic episodes lasting for more than 6 hours by cooling of the penis and perineum, and walking upstairs [1572]. In SCD patients with priapism, it is recommended that the urology team works closely with the haematology team to optimise patient management.
Partial priapism usually resolves spontaneously with analgesic treatment while surgical intervention is rarely needed [1591].
10.1.3.1.2. Penile anaesthesia/analgesia
It is possible to perform blood aspiration and intracavernous injection of a sympathomimetic agent without any anaesthesia. However, anaesthesia may be necessary when there is severe penile pain. While it is recognised that the anaesthesia may not alleviate the ischaemic pain, cutaneous anaesthesia facilitates subsequent therapies. The treatment options for penile anaesthesia/systemic analgesia include:
- dorsal nerve block;
- circumferential penile block;
- subcutaneous local penile shaft block;
- oral conscious sedation (for paediatric patients).
10.1.3.1.3. Aspiration ± irrigation with 0.9% w/v saline solution
The first intervention for an episode of priapism lasting more than 4 hours consists of corporal blood aspiration (LE: 4) to drain the stagnant blood from the corporal bodies, making it possible to relieve the compartment-syndrome-like condition within the corpus cavernosum. Blood aspiration may be performed with intracorporeal access either through the glans or via percutaneous needle access to the lateral aspect of the proximal penile shaft, using a 16 or 18 G angio-catheter or butterfly needle. The needle must penetrate the skin, the subcutaneous tissue and the tunica albuginea to drain blood from the corpus cavernosum (LE: 4).
Some clinicians advocate using two angiocatheters or butterfly needles at the same time to accelerate drainage, as well as aspirating and irrigating simultaneously with a saline solution [1572] (LE: 4). Aspiration should be continued until bright red, oxygenated blood is aspirated (LE: 4).
Several case series have reported the outcomes from first-line treatments, although in most cases, aspiration and irrigation were combined with intracavernosal injection of sympathomimetic agents, thus making it difficult to draw conclusions about the success rate of aspiration + irrigation alone. In a RCT, 70 patients with ischaemic priapism secondary to intracavernosal injection and lasting more than 6 hours were treated with aspiration plus saline irrigation at different temperatures [1572]. The authors reported an 85% success rate with the optimum results achieved using a 10°C saline infusion after blood aspiration.
This approach has up to a 30% chance of resolving the priapism. There are insufficient data to determine whether aspiration followed by saline intracorporeal irrigation is more effective than aspiration alone (LE: 4).
10.1.3.1.4. Aspiration ± irrigation with 0.9% w/v saline solution in combination with intracavernous injection of pharmacological agents
This combination is currently considered the standard of care for treatment of ischaemic priapism [1555,1592,1593] (LE: 4). Pharmacological agents include sympathomimetic drugs or α-adrenergic agonists. Intracavernous sympathomimetic agents include phenylephrine, etilephrine, ephedrine, epinephrine, norepinephrine and metaraminol with a resolution rate of up to 80% [1555,1592,1594-1601] (LE: 2b). The use of intracavernous adrenaline injection alone has also been sporadically reported [1602]. A literature review from the American Urological Association (AUA) reported that the use of a sympathomimetic agent combined with prior intracavernosal aspiration or irrigation had a resolution rate of 77% as compared with 58% in those who had a sympathomimetic injection alone [1593].
Phenylephrine
Adrenergic agonists act on the post-synaptic α-1-adrenergic receptors to stimulate cavernosal smooth muscle and arteriolar vasoconstriction, with a reduction in arteriolar inflow to the corporal bodies and smooth muscle contraction [1603]. Moreover, this class of drug also increases venous outflow through β2-adrenergic receptor activity [1600].
Phenylephrine is a selective α-1-adrenergic receptor agonist that has been observed in small case series to be effective at producing detumescence in priapism, when given as an intracavernosal injection, with few adverse effects [1600,1604]. Therefore, phenylephrine is the recommended adrenergic agonist drug of choice due to its high selectivity for the α-1-adrenergic receptor, without concomitant β-mediated inotropic and chronotropic cardiac effects [1594,1598,1599] (LE: 4).
Phenylephrine is diluted in normal saline to a concentration of 100-500 μg/mL. Usually, 200 μg are given every three to five minutes directly into the corpus cavernosum. The maximum dosage is 1 mg within 1 hour (LE: 4). A lower concentration or volume is applicable for children and patients with severe cardiovascular diseases (LE: 4).
Higher doses of phenylephrine have been used in small retrospective case series [1598,1599,1605,1606] without any adverse events, but further trials are needed to substantiate the efficacy of higher doses. There are in-vitro data suggesting that higher doses of phenylephrine are unlikely to be beneficial when conventional doses have failed because there is already significant apoptosis of the cavernosal smooth muscle [1607].
Phenylephrine has potential cardiovascular adverse effects [1555,1592,1594,1595,1598,1599] and it is recommended that blood pressure and pulse are monitored every fifteen minutes for 1 hour after injection. This is particularly important in older men with pre-existing cardiovascular diseases. After injection, the puncture site should be compressed and the corpus cavernosum massaged to facilitate drug distribution.
The potential treatment-related adverse effects of intracavernous phenylephrine (and other sympathomimetic agents) include headache, dizziness, hypertension, reflex bradycardia, tachycardia and palpitations and sporadic subarachnoid haemorrhage [347]. Monitoring of blood pressure and pulse should be performed during intracavernous administration of sympathomimetic agents.
Given that intracavernous sympathomimetic agents can cause hypertension, the Panel is of the opinion that these agents are contraindicated in patients with malignant or poorly controlled hypertension, as there are case reports of significant cardiovascular and neurological complications following the use of these pharmacological agents for priapism [1595,1608,1609]. Similarly, there are data suggesting that sympathomimetic agents cause a hypertensive crisis when given with monoamine oxidase inhibitors, hence these medications should not be used together [1610] (LE: 4).
Etilephrine
Etilephrine is also an adrenergic agonist but directly stimulates both α and β adrenergic receptors [1593]. Most of the literature describing the use of etilephrine for treatment of priapism is related to men with SCD but there are small retrospective case series that have reported its benefits for priapism secondary to iatrogenic causes [1611,1612]. Etilephrine is the second most widely used sympathomimetic agent, administered by intracavernous injection at a concentration of 2.5 mg in 1-2 mL normal saline [1595] (LE: 3).
Methylene blue
Methylene blue is a guanylate cyclase inhibitor, that may be a potential inhibitor of endothelial-mediated cavernous smooth muscle relaxation. Small retrospective case series have reported its successful use for treating short-term pharmacologically-induced priapism [1613,1614] (LE: 3). Methylene blue, 50-100 mg
[1613], should be injected intracavernously and left for five minutes. It is then aspirated and the penis compressed for an additional five minutes [1614]. Treatment-related adverse effects include a transient burning sensation and blue discolouration of the penis.
Adrenaline
Adrenaline produces both α-adrenergic receptor agonist and β-adrenergic receptor activity. Intracavernosal adrenaline (2 mL of 1/100,000 adrenaline solution up to five times over a 20-minute period [1602]) has been used in patients with ischaemic priapism due to an intracavernous injection of vasoactive agents. The limited literature [1602,1615] suggests that adrenaline can achieve detumescence in short-term priapism, with one small case series reporting a success rate of over 50% after a single injection, with an overall success rate of 95% with repeated injections [1602,1615] (LE: 3).
β-2-agonists
Oral terbutaline is a β-2-agonist with minor β-1 effects and some α-agonist activity. A dose of 5 mg has been suggested to treat prolonged erections lasting more than 2.5 hours, after intracavernous injection of vasoactive agents, although the mechanism of action is not yet fully understood [1616-1618] (LE: 1b). The main use of terbutaline is for prevention of recurrent episodes of prolonged erection. Terbutaline should be given cautiously in patients with coronary artery disease, increased intravascular fluid volume, oedema or hypokalaemia [1618]. In a single multi-centre prospective study, another β-2-agonist, salbutamol, has been reported to induce detumescence in 34% of cases of prolonged erection (more than 3 hours) after intracavernous injection of erectogenic agents [1619]. However, more robust data are needed to recommend oral salbutamol for the treatment of ischaemic priapism.
Anti-thrombotic agents
Ramstein et al. reported retrospective data pertaining to the use of antithrombotic therapy (a single dose of subcutaneous heparin or aspirin 325 mg) in patients who had undergone corporeal aspiration with and without phenylephrine. Antithrombotic therapy was associated with a significant reduction in further episodes of priapism following aspiration and successful T-shunt insertions in those who failed aspiration. However, these findings were based on a small cohort size (n = 18), doses and types of antithrombotic therapy were heterogeneous, and exact timing of the priapism episodes was not measured precisely. In this setting, further prospective randomised trials are needed prior to the recommendation of antithrombotic agents for treatment or adjunctive therapy of ischaemic priapism [1620].
Table 49: Medical treatment of ischaemic priapism
Drug | Dose/Instructions for use |
Phenylephrine |
|
Etilephrine |
|
Methylene blue |
|
Adrenaline |
|
Terbutaline |
|
Management of priapism related to sickle cell disease
The Panel conducted a systematic review on the overall management of priapism related to SCD. Unfortunately, few studies were conducted exclusively on patients with SCD and studies on mixed populations usually did not report separate data on SCD patients. Clear and systematic reporting of patient characteristics, interventions and outcomes was lacking, and the length of follow-up, if reported, varied significantly among the studies. Overall, the quality of studies was deemed poor for high-quality, evidence-based recommendations.
Urgent intervention is essential (LE: 4) and the general approach is similar to that described for other cases of ischaemic priapism and should be co-ordinated with a haematologist [1607,1621,1622] (LE: 4).
However, as with other haematological disorders, other therapeutic interventions may also need to be implemented [1621-1623]. Specific measures for SCD-related priapism include intravenous hydration and narcotic analgesia while preparing the patient for aspiration and irrigation. Additionally, supplemental oxygen administration and alkalinisation with bicarbonate can be helpful [1573,1607].
Haemoglobin S (HbS) percentage should be measured in all SCD patients with acute priapism. Exchange blood transfusion has also been proposed, with the aim of increasing tissue delivery of oxygen [1624]. The transfused blood should be sickle cell haemoglobin negative and Rh and Kell antigen matched [1625]. However, the evidence is inconclusive as to whether exchange transfusion itself helps to resolve priapism. A systematic review reported that the mean time to detumescence was eleven days with exchange transfusions compared to eight days with conventional treatment. Moreover, there were 9 cases of ASPEN syndrome (association of SCD, priapism, exchange transfusion and neurological events) as a consequence of blood transfusion [1626].
Consensus recommendation: exchange transfusion should not be used as a primary treatment for ischaemic priapism in patients with SCD.
Several reports suggest that exchange transfusion may result in serious neurological sequelae [1626], although a series of 10 patients with SCD-related priapism showed that it was safe to perform exchange transfusion [1624]. Because of these considerations, routine use of exchange transfusion is not recommended as a primary treatment intervention in this group unless there is a risk of SCD-related symptoms (LE: 4). However, in patients who fail medical management, transfusion may be required to enable general anaesthesia to be safely administered prior to definitive surgery [1627].
10.1.3.2. Surgical management
Evidence acquisition
The majority of the identified studies for surgical management were retrospective and non-randomised. A significant proportion of the reports were case series reporting on one or two particular types of surgical procedures, often with low patient numbers (< 20) (Appendix 2 online supplementary evidence). The studies showed a wide variation in data, including the proportion of patients who had prior conservative management, reporting of initial success, and duration of follow-up. Surgical complications were also not consistently reported. The systematic review captured specific end points of priapism resolution, sexual function and surgical adverse events when reported. However, due to the heterogeneity of the data, direct comparisons of success rates and long-term outcomes should be treated with caution.
10.1.3.2.1. Second-line treatments
Second-line intervention typically refers to surgical intervention in the form of penile shunt surgery and penile implant insertion for refractory or delayed ischaemic priapism, and should only be considered when other conservative management options fail (LE: 4). There is no evidence detailing the time frames before moving on to surgery after first-line treatment, although a period of at least 1 hour of first-line treatment without detumescence can be considered prior to moving to surgical intervention (LE: 4).
A number of clinical indicators suggest failure of first-line treatment including continuing corporal rigidity, cavernosal acidosis, anoxia, severe glucopenia, absence of cavernosal artery inflow by penile colour duplex US, and elevated intracorporal pressure [1628]. Colour duplex US of the penis in the ischaemic state may be helpful but it should be noted that blood flow may persist in the tumescent phase of erection [1629] (LE: 4).
10.1.3.2.1.1. Penile shunt surgery
Penile shunt surgery aims to produce an outflow for ischaemic blood from the corpus cavernosum into the corpus spongiosal tissues, thereby allowing restoration of normal circulation within these structures. Accordingly, a shunt creates an opening in the tunica albuginea, with either the glans, corpus spongiosum, or a vein for blood drainage (Table 50) [1555,1592,1630].
The type of shunt procedure is chosen according to the surgeon’s preference and familiarity with the procedure. It is conventional for distal shunt procedures to be tried before considering proximal shunting (LE: 4). Gadolinium-enhanced penile MRI [1588] and cavernosal smooth muscle biopsy have been used to diagnose smooth muscle necrosis (which, if present, would suggest that shunting is likely to fail) and may help in decision-making and patient counselling in cases of refractory or delayed presentation (> 48 hours) that may be considered for immediate penile prosthesis insertion (see below).
It is important to assess the success of surgery by direct observation of penile rigidity or by repeated testing (e.g., cavernous blood gas testing) (LE: 4) [1555,1592,1631,1632]. The use of penile colour duplex US may not give appropriate information because of the hyperaemic (reperfusion) period that follows decompression after the ischaemic state [1629].
The recovery rates of erectile function in men undergoing shunt surgery following prolonged episodes of priapism are low and are directly related to the duration of priapism, pre-operative erectile status and age [1631-1633]. The exact duration of priapism for shunt surgery to preserve erectile function is not based on studies with high levels of evidence. If ischaemic priapism resolves within 24 hours of onset, it has been reported that 78-100% of patients regain spontaneous functional erections (with or without PDE5Is use). In contrast, other studies have shown that priapism for more than 36-48 hours appears to result in both structural and functional effects on corporal smooth muscle, with poorer outcomes (ED > 90%) [1631,1634]. In general, shunt procedures undertaken after this time period (36-48 hours) may only serve to limit pain without any beneficial effects on erectile function and early prosthesis insertion can be considered [1562,1635].
Four categories of shunt procedures have been reported [1555,1593,1630,1635]. The limited available data preclude any overall recommendation for one procedure over another based upon outcomes, but distal shunts are less invasive and associated with lower rates of post-operative ED and therefore are recommended as the first surgical intervention of choice (Table 50) (LE: 4).
Percutaneous distal (corpora-glanular) shunts
Winter’s procedure uses a Trucut biopsy needle to create a fistula between the glans penis and each corpus cavernosum [1555,1569,1593,1629,1636] (LE: 3). Post-operative sequelae are uncommon [1637]. Winter’s shunt is easy to perform, but has been reported as the least successful operation to create a distal shunt [1632]. This is because the diameter of the Trucut needle is only 1.6 mm (14-18 g) and therefore cannot accommodate the increased blood flow from post-ischaemic hyperaemia, resulting in poor drainage, increased intracavernous pressure and consequent premature closure of the shunt [1629].
Ebbehoj’s technique involves making multiple tunical incision windows between the glans and each tip of the corpus cavernosum by means of a size 11 blade scalpel passed several times percutaneously [1555,1593,1629,1638,1639] (LE: 3).
T-Shunt involves performing a bilateral procedure using a scalpel with a size 10 blade inserted through the glans just lateral to the urethral meatus until it enters the tip of the corpus cavernosum. The blade is then rotated 90° away (to the lateral side) from the urethral meatus and withdrawn [1555,1593,1629,1640] (LE: 3). If unsuccessful, the procedure is repeated on the opposite side. The T-shunt can be followed by a tunnelling procedure using a size 8/10 Hegar dilator inserted through the glans and into the corpus cavernosum, which can also be performed using US guidance, mainly to avoid urethral injury [1640]. The entry sites in the glans are sutured following detumescence. Tunnelling with a 7 mm metal sound or 7/8 Hegar dilator is necessary in patients with priapism duration > 48 hours. Tunnelling is a potentially attractive procedure as it combines the features of distal and proximal shunts with proximal drainage of the corpus cavernosum and may ameliorate the profibrotic effect of sludged blood retained in the corpus cavernosum [1633,1635,1640].
Open distal (corpora-glanular) shunts
Al-Ghorab’s procedure consists of an open bilateral excision of circular cone segments of the distal tunica albuginea via the glans penis, along with subsequent glans closure by running suture with absorbable material. A transverse incision on the glans may compromise arterial blood flow because distal deep dorsal arteries run longitudinally in the glans [1555,1593,1629,1641-1643] (LE: 3).
Burnett’s technique (Snake manoeuvre) is a modification of the Al-Ghorab corpora-glanular shunt. It involves retrograde insertion of a 7/8 Hegar dilator into the distal end of each corpus cavernosum through the original Al-Ghorab glanular excision. After removal of the dilator from the corpus cavernosum, blood evacuation is facilitated by manual compression of the penis sequentially from a proximal to distal direction. After detumescence, the glans penis is closed as in the Al-Ghorab procedure [1555,1593,1629,1644,1645] (LE: 3). Reported complications include wound infection, penile skin necrosis and urethrocutaneous fistulae [1645].
Table 50: Distal shunt procedures in ischaemic priapism
Study | N: (shunt/shunt + tunnelling) | Duration of priapism (shunt/shunt + tunnelling) | Type of surgery | Detumescence rate (shunt/shunt + tunnelling) | Post-operative ED rate (shunt/shunt + tunnelling) |
Ercole et al. [1641] | 7 (7/0) | 2.6 d / NA | Al-Ghorab | 100% / NA | 57% / NA |
Macaluso et al. [1637] | 12 (12/0) | 58 h / NA | Winter | 100% / NA | 17% / NA |
Nixon et al. [1632] | 14 (14/0) | 42 h / NA | Winter | 14% / NA | 90% / NA |
Lund et al. [1639] | 18 (18/0) | 20 h to 8 months / NA | Ebbehoj | 61% / NA | 39% / NA |
Brant et al. [1640] | 13 (6/7) | 50 h / 80 h | T-shunt/T-shunt + tunnelling | 46% / 92% | 16% / 57% |
Segal et al. [1645] | 10 (0/10) | NA / 60 h | Al-Ghorab + tunnelling | NA / 80% | NA / 40% |
Zacharakis et al. [1635] | 45 (0/45) | NA / 96 h | T-shunt + tunnelling | NA / 64% | NA / 93% |
Ortaç et al. [1633] | 19 (6/13) | 48h / 70h | T-shunt/T-shunt + tunnelling | 31% / 94% | 83% / 85% |
Summary | 138 (63/75) | 52h / 76h | - | 60% / 82% | 50% / 68% |
ED = erectile dysfunction; h = hours; d = days.
Open proximal (corpora-spongiosal) shunts
Quackles’s technique uses a trans-scrotal or perineal approach; a proximal open shunt technique creates a communication between the corpus cavernosum and the corpus spongiosum. The most frequent complications include an unwanted urethro-cavernous fistula and urethral stricture or cavernositis [1555,1593,1630,1646]. The risk of urethral injury is less with a perineal approach to the bulb of the corpus spongiosum (LE: 3). Proximal shunts are more invasive and ED rates are documented to be higher [1628].
Peno-scrotal decompression
More recently a proximal decompression technique with the aim to spare the glans with high success rates has been described. The technique is based upon opening of the proximal corpus cavernosum combined with proximal and distal tunnelling using a suction tip [1647]. In a cohort of 25 patients, 12 had undergone previous corpora-glanular shunt surgery. Recurrence was observed in two of 25 patients with unilateral peno-scrotal decompression. In the 15 patients who had follow-up data, 40% had ED. Whilst, representing a promising technique, PSD in cases of refractory priapism may further delay penile prosthesis insertion with detrimental effects on surgical outcomes including penile shortening and prosthetic infection.
Anti-thrombotic agents
Procedures for shunting require incision through the tunica albuginea and expose collagen to coagulation factors in the penile blood and thus activate the blood-clotting cascade. Peri-operative anti-coagulation is advocated to facilitate resolution of the priapism. There was an 84% decrease in priapism recurrence in the shunt group that received peri-procedural anti-thrombotic treatment (325 mg acetylsalicylic acid pre-operatively, and 5000 IU intraoperative heparin, post-operatively for 5 days (81 mg acetylsalicylic acid and
75 mg clopidogrel) compared with the group that did not receive peri-procedural anti-thrombotic treatment after failed aspiration [1620].
Vein anastomoses/shunts
Grayhack’s procedure mobilises the saphenous vein below the junction of the femoral vein and anastomoses the vein end-to-side onto the corpus cavernosum. Venous shunts may be complicated by saphenofemoral thrombus formation and by pulmonary embolism [1555,1593,1648-1650] (LE: 3).
Immediate penile prosthesis implantation
The literature pertaining to penile implantation surgery is shown in Appendix 3 online supplementary evidence. The studies identified here were principally retrospective non-randomised case series. In all but one study, patients had prior non-surgical management. All of the studies described priapism resolution rate, sexual function and surgical adverse events although the follow-up period was variable.
Refractory, therapy-resistant, acute ischaemic priapism or episodes lasting more than 48 hours usually result in complete ED, possibly along with significant penile deformity in the long-term. In these cases, immediate penile prosthesis surgery is advocated [1651-1654] (LE: 3).
The immediate insertion of a malleable penile prosthesis is recommended to avoid the difficulty and complications of delayed prosthetic surgery in the presence of corporal fibrosis. Potential complications that could compromise immediate penile prosthesis implantation include distal erosion and infection [1651,1653], along with a small rate of revision surgery [1651]. Early surgery also offers the opportunity to maintain penile length and girth and prevent penile curvature due to cavernosal fibrosis. The prosthesis can be exchanged for an inflatable prosthesis at a later date, which may allow upsizing of the implant cylinders [1655].
Currently, there are no clear indications for immediately implanting a penile prosthesis in men with acute ischaemic priapism, although this can be considered in men with delayed or refractory priapism (see below [1592]).
Consensus recommendation (LE: 4):
Relative indications include:
- Ischaemia that has been present for more than 48 hours.
- Failure of aspiration and sympathomimetic intracavernous injections in delayed priapism (> 48 hours).
- Magnetic resonance imaging or corporal biopsy evidence of corporal smooth muscle necrosis [1555,1651] (LE: 4).
- Failure of a shunting procedure [although in delayed cases (> 48 hours), implantation might be considered ahead of shunt surgery].
- Refractory priapism in patients who have undergone shunting procedures.
The optimal time for implantation is within the first three weeks from the priapism episode [1562,1628,1656]. If shunt surgery has been performed, penile prosthesis implantation can be further delayed in order to allow reduction of oedema, wound healing and risk of prosthetic infection. A vacuum device to avoid fibrosis and penile shortening may be used during this waiting period [1657].
The decision on which type of implant to insert is dependent on patient suitability, surgeons’ experience, and availability and cost of the equipment. There are no randomised trials comparing the efficacy and complication rates of malleable and inflatable penile prostheses. Despite the higher infection rate in priapism patients compared to those with virgin prosthesis, in patients who are well-motivated and counselled prior to the procedure, immediate inflatable penile prosthesis implantation may be undertaken, although in most cases a semi-rigid implant is more suitable as it is easier to implant and reduces operative time and hence the risk of prosthetic infection. A further issue with immediate insertion of an inflatable penile prosthesis is that the patient must begin cycling the device immediately to avoid a fibrous capsule forming and contracting. Early cycling of an inflatable penile prosthesis prevents penile curvature and shortening [1562].
Surgery for non-acute sequelae after ischaemic priapism
Structural changes may occur after ischaemic priapism including cavernosal tissue necrosis and fibrosis with consequent penile scarring, megalophallic deformities, penile shortening, and occasional penile loss [1630,1651,1658,1659]. Erectile dysfunction is also often observed [1555,1660]. Unfortunately, these outcomes can still occur despite apparently successful first-line or second-line treatment in detumescence of the penis.
Penile prosthesis implantation is occasionally indicated in SCD patients with severe ED because other therapeutic options, such as PDE5Is and intracavernous injections are avoided as they may provoke a further priapism event [1555,1592]. In severe corporal fibrosis, narrow-based prosthetic devices are preferable because they are easier to insert and need less dilatation [1651] (LE: 3). After severe priapism that has resulted in penile destruction with complicated deformities or even loss of penile tissue, it may be necessary to make changes to the surgical technique. Multiple corporotomies, corporal excavation, optical corporotomy-Shaeer technique, dilatation with Carrion-Rosello cavernotome, Uramix or Mooreville cavernotome, excision of scar tissue, and use of small-diameter prosthesis, or penile reconstruction using grafts can be utilised, if concomitant prosthesis implantation is considered [1634,1661] (LE: 3). Early implantation of a penile prosthesis is associated with lower infection rates (6-7% vs. 19-30%), penile shortening (3% vs. 40%) and revision rates (9% vs. 27%) compared to late insertion. General satisfaction rate for early implantation is higher (96%) than for late implantation (60%) [1562] (Appendix 4 online supplementary evidence).
Figure 15: Algorithm on surgical management of priapism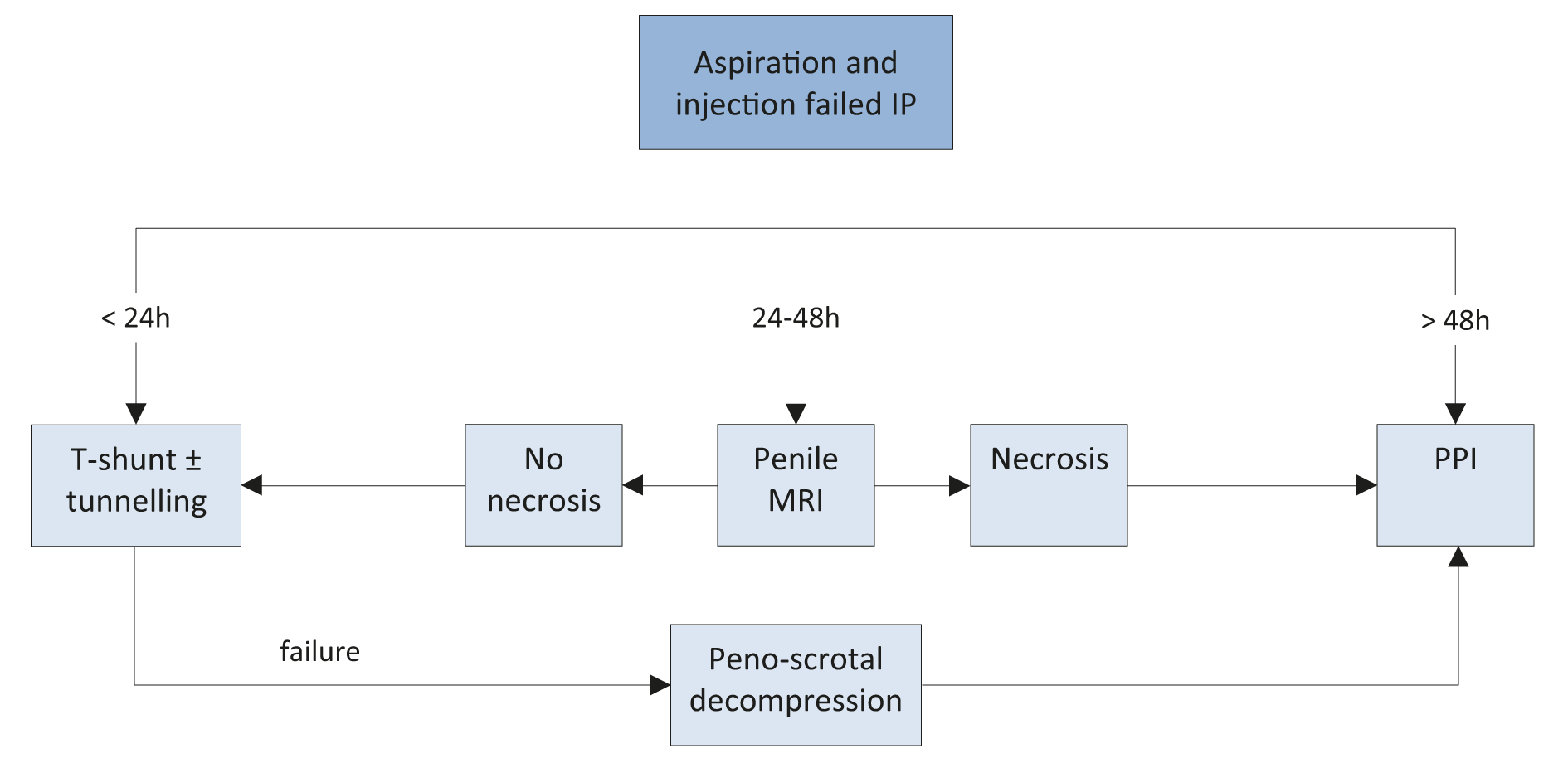 IP = ischaemic priapism; MRI = Magnetic resonance imaging; PPI = penile prosthesis implantation.
IP = ischaemic priapism; MRI = Magnetic resonance imaging; PPI = penile prosthesis implantation.
10.1.4. Summary of evidence for treatment of ischaemic priapism
Summary of evidence | LE |
Emergency intervention for ischaemic priapism is mandatory. | 2b |
The aim of treatment is to facilitate painless penile detumescence, to prevent chronic fibrosis of the corpus cavernosum. | 3 |
Erectile function preservation is directly related to the duration of ischaemic priapism, age and pre-operative erectile status. | 2b |
Phenylephrine is the recommended drug due to its favourable safety profile in the cardiovascular system compared to other drugs. Phenylephrine is usually diluted in normal saline with a concentration of 100-500 μg/mL and given in 200 μg doses every three to five minutes directly into | 2b |
Gadolinium-enhanced MRI may be useful to diagnose smooth muscle necrosis in cases of delayed or refractory priapism. | 3 |
Shunt procedures are effective to resolve priapism and provide pain relief. No clear recommendation of the superiority of one type of shunt over another can be given. Distal shunts are less invasive and associated with lower rate of erectile dysfunction. | 2b |
Peri- and post-operative anticoagulant prophylaxis (325 mg acetylsalicylic acid pre-operatively, 5,000 IU heparin intra-operatively and 81 mg acetylsalicylic acid and 75 mg clopidogrel five days post-operatively) may prevent priapism recurrence. | 3 |
Erectile dysfunction is almost inevitable in prolonged cases or ischaemic priapism. Early implantation of penile prosthesis is associated with lower infection rates and complications compared to late implantation. | 2b |
10.1.5. Recommendations for the treatment of ischaemic priapism
Recommendations | Strength rating |
Start management of ischaemic priapism as early as possible (within four to six hours) and follow a stepwise approach. | Strong |
First, decompress the corpus cavernosum by penile aspiration and washout until fresh red blood is obtained. | Strong |
In priapism secondary to intracavernous injections of vasoactive agents, replace blood aspiration with intracavernous injection of a sympathomimetic drug as the first step. | Strong |
In priapism that persists despite aspiration, proceed to the next step, which is intracavernous injection of a sympathomimetic drug. | Strong |
In cases that persist despite aspiration and intracavernous injection of a sympathomimetic drug, repeat these steps before considering surgical intervention. | Strong |
Treat ischaemic priapism associated with sickle cell disease in the same fashion as idiopathic ischaemic priapism. Provide other supportive measures (intravenous hydration, oxygen administration with alkalisation with bicarbonate, blood exchange transfusions), but do not delay initial treatment to the penis. | Strong |
Proceed to surgical treatment only when blood aspiration and intracavernous injection of sympathomimetic drugs have failed. | Strong |
Perform distal shunt surgical procedures first and combine them with tunnelling if necessary. | Weak |
Proximal procedures may be used in cases of distal shunt failure (< 48 hours) or in patients who do not wish to proceed with immediate penile implant insertion. | Weak |
Peri- and post-operative anticoagulation may decrease priapism recurrence. | Weak |
A penile prosthesis may be preferred over proximal shunting particularly in delayed > 48 hours) or refractory priapism. | Weak |
Implantation of a prosthesis may be considered in delayed presentation (> 48 hours) and in those cases refractory to injection therapy and distal shunting. | Weak |
If a shunt has been performed, then implantation of a penile prosthesis should be delayed to minimise the risk of infection and erosion of the implant. | Strong |
The decision on which type of implant to insert is dependent on patient suitability, surgeons’ experience and availability and cost of the equipment. If malleable penile prosthesis is implanted it can be later exchanged to an ınflatable penıle implant. | Strong |
Patients must be fully counselled regarding the risks and benefits of implant insertion in cases of delayed presentation of refractory priapism. | Weak |
10.2. Priapism in Special Situations
10.2.1. Stuttering (recurrent or intermittent) priapism
10.2.1.1. Epidemiology/aetiology/pathophysiology
Robust epidemiological studies of stuttering priapism are lacking [1662,1663]. However, recurrent priapism episodes are common in men with SCD (42-64%) [1664,1665] while in adolescents and young men the incidence of priapism is 35%, of whom 72% have a history of stuttering priapism [1662].
The aetiology of stuttering priapism is similar to that of ischaemic priapism. Whilst SCD is the most common cause, idiopathic cases and cases due to a neurological disorder have been reported. Men who have acute ischaemic priapism, especially which has been prolonged (for more than 4 hours) are at risk of developing stuttering priapism [1660].
Several studies have proposed alternative mechanisms for stuttering priapism including inflammation, cellular adhesion, NO metabolism, vascular reactivity and coagulation [1555,1574,1607,1666,1667]. Specifically, a deficiency in endothelial NO causes downregulation in a cyclic guanosine monophosphate (cGMP)-dependent protein kinase and PDE5, resulting in dysregulation in the corporal smooth muscle tone [1668]. Furthermore, decreased NO availability decreases RhoA (Ras homolog gene family) and Rho-kinase, which are important factors for penile detumescence, and disrupts adenosine signalling [1669]. The lack of mechanisms to regulate cGMP, along with reduced vasoconstriction, reduce cavernosal smooth muscle tone, leading to an increased and disproportionate response to stimuli. Adenosine, like NO, is a potent vasodilator and regulator of penile tumescence. It is increased in conditions of stress, hypoxia and ischaemia, suggesting an important role in the pathogenesis of the priapic state [1670]. Finally, although debated, androgens have also been observed to have an association with priapism [1671]. Androgens play an important role in the mediation of erections both centrally and peripherally. They are known to contribute toward the regulatory basis of both NO synthase and PDE5 expression and activity in various structures of the local erectile apparatus [1672]. Therefore, one of the options for the treatment of stuttering priapism is to reduce serum testosterone levels to hypogonadal levels, which then suppresses androgen-associated mechanisms believed to be involved in triggering recurrent priapism.
10.2.1.1.1. Summary of evidence on the epidemiology, aetiology and pathophysiology of stuttering priapism
Summary of evidence | LE |
Stuttering priapism is similar to ischaemic priapism in that it is low-flow and ischaemic and, if left untreated, can result in significant penile fibrosis, with SCD being the most common cause. | 3 |
10.2.1.2. Classification
Stuttering priapism, also termed intermittent or recurrent priapism, is a distinct condition that is characterised by repetitive and painful episodes of prolonged erections. Erections are self-limiting with intervening periods of detumescence [1607,1666]. These are analogous to repeated episodes of ischaemic priapism. In stuttering priapism the duration of the erections is generally shorter than in ischaemic priapism [1593]. The frequency and/or duration of these episodes is variable and a single episode can sometimes progress into prolonged ischaemic priapism.
10.2.1.3. Diagnostic evaluation
10.2.1.3.1. History
A comprehensive history is mandatory and follows the same principles as described in Table 46. There is a history of recurrent episodes of prolonged erections. These episodes can occur from several daily to isolated incidents every few months, continuously or followed by incident-free periods, of unknown duration, even months and years [1673]. The onset of the priapic episodes usually occurs during sleep and detumescence does not occur upon waking. These episodes can be painful and may be the reason that the patient first seeks medical attention. Priapism can cause significant impairment of mental health with patients experiencing sadness, embarrassment, fear, and exhaustion [1674].
10.2.1.3.2. Physical examination
Erections are painful and the penis is rigid as in ischaemic priapism, but the duration of events is usually shorter. Between erections the penis is usually normal, but in some cases signs of fibrosis can be found. Rarely, the penis may become enlarged, a condition known as megalo-phallus.
10.2.1.3.3. Laboratory testing
Laboratory testing follows the same principles as in the two other types of priapism. It is recommended to identify possible causes and should be directed by the history and clinical and laboratory findings.
10.2.1.3.4. Penile imaging
There are no specific findings on imaging for stuttering priapism. Colour duplex US of the penis and perineum and MRI are recommended and can differentiate non-ischaemic from ischaemic forms of priapism.
10.2.1.3.5. Recommendations for diagnosis of stuttering priapism
The same recommendations as described in Section 10.1.2.5 apply. Stuttering priapism is a recurrent or intermittent type of ischaemic priapism.
10.2.1.4. Disease management
The primary goal in the management of patients with stuttering priapism is the prevention of further episodes and limiting the chances of developing a prolonged ischaemic priapism that is refractory to conventional treatment options. In most cases, stuttering priapism can be managed by pharmacological treatment, the aim of which is to reduce the frequency and severity of stuttering episodes. The management of each acute episode is similar to that for ischaemic priapism; aspiration/irrigation in combination with intracavernous injections of α-adrenergic agonists. Unfortunately, the efficacy and safety of the various treatment modalities suggested in the medical literature are poorly reported. Specifically, most reports are from small case series and the Panel is not aware of any published, well-designed, controlled studies on the efficacy and safety of these treatments [1573,1607,1666,1673].
10.2.1.4.1.α-Adrenergic agonists
Studies of oral α-adrenergic agonists have suggested some prophylactic benefit for daily treatment with these agents [1675]. Adverse effects include tachycardia and palpitations. Pseudoephedrine is widely used as an oral decongestant and can be a first-line treatment option for stuttering priapism [1617]. However, its effect on corporal smooth muscle is not fully understood. Etilephrine has been used successfully to prevent stuttering priapism caused by SCD. It is usually taken orally at doses of 5-10 mg daily, with response rates of up to 72% [1676-1678]. In one randomised, placebo-controlled clinical study comparing medical prophylaxis with etilephrine and ephedrine, there was no difference in efficacy between the two drugs.
10.2.1.4.2. Hormonal manipulations of circulating testosterone
The aim of hormonal manipulation is to down-regulate circulating testosterone levels to suppress the action of androgens on penile erection [1573,1607,1679]. This can be achieved by GnRH agonists or antagonists, antiandrogens or oestrogens [1680,1681] (LE: 4). Potential adverse effects may include hot flushes, gynaecomastia, ED, loss of libido, and asthenia. All approaches have a similar efficacy profile (LE: 4) while the potential cardiovascular toxicity of oestrogens limits their clinical use. Alternative endocrine approaches that have been used with some success include 5-α-reductase inhibitors [1682,1683] (LE: 3) and ketoconazole; an anti-fungal agent that reduces adrenal and testicular androgen production [1679,1684] (LE: 4).
The duration of hormonal treatment for effective suppression of recurrent priapism is problematic. It is not possible to draw any conclusions on the dose, duration of treatment and the efficacy. Caution is strongly advised when prescribing hormonal treatments to pre-pubertal boys and adolescents, and specialist advice from paediatric endocrinologists should be sought. Likewise, hormonal agents have a contraceptive effect and interfere with normal sexual maturation and spermatogenesis and affect fertility. Therefore, men who are trying with their partner to conceive should be comprehensively counselled before using hormonal treatment. Moreover, sperm cryopreservation may be considered to mitigate any potential effects of anti-androgen therapy on fertility.
10.2.1.4.3. Digoxin
Digoxin is a cardiac glycoside and positive inotrope that is used to treat congestive heart failure. Digoxin regulates smooth muscle tone through several different pathways leading to penile detumescence [1573,1607,1685]. The use of maintenance digoxin doses (0.25-0.5 mg/daily) in idiopathic stuttering priapism reduces the number of hospital visits and improves QoL [1607]. In a small, clinical, double-blind, placebo-controlled study, digoxin decreased sexual desire and excitement with a concomitant reduction in penile rigidity, regardless of any significant change in plasma levels of testosterone, oestrogens and LH [1685] (LE: 2b). Adverse effects include decreased libido, anorexia, nausea, vomiting, confusion, blurred vision, headache, gynaecomastia, rash and arrhythmia.
10.2.1.4.4. Terbutaline
Terbutaline is a β-agonist that causes vasodilation, resulting in vascular smooth muscle relaxation [1573,1607] and has been used to prevent stuttering priapism with detumescence rates of 36% in patients with alprostadil-induced priapism [1617] (LE: 3). The only randomised, placebo-controlled study (n = 68) in patients with pharmacologically-induced priapism, demonstrated detumescence in 42% of the terbutaline-treated group compared to only 15% in the placebo-treated group [1618] (LE: 1b). Adverse effects include nervousness, shakiness, drowsiness, palpitations, headache, dizziness, hot flushes, nausea and weakness.
10.2.1.4.5. Gabapentin
Gabapentin has anticonvulsant, antinociceptive and anxiolytic properties and is widely used as an analgesic and anti-epileptic agent. Its proposed mechanism of action is to inhibit voltage-gated calcium channels, which attenuates synaptic transmission [1679], and reduces testosterone and FSH levels [1686]. It is given at a dose of 400 mg, four times daily, up to 2,400 mg daily, until complete penile detumescence occurs, with subsequent maintenance administration of 300 mg/daily [1687] (LE: 4). Adverse effects include anorgasmia and impaired erectile function.
10.2.1.4.6. Baclofen
Baclofen is a gamma-aminobutyric acid (GABA) derivative that acts as a muscle relaxant and anti-muscle spasm agent. It can inhibit penile erection and ejaculation through GABA activity and prevents recurrent reflexogenic erections or prolonged erections from neurological diseases [1573]. Oral baclofen has little efficacy and it is not usually used in stuttering priapism but intrathecal administration is more effective [1607,1688-1690] (LE: 4). Adverse effects include drowsiness, confusion, dizziness, weakness, fatigue, headache, hypotension and nausea.
10.2.1.4.7. Hydroxyurea
Hydroxyurea blocks the synthesis of deoxyribonucleic acid (DNA) by inhibiting ribonucleotide reductase, which has the effect of arresting cells in the S-phase [1679,1691]. Hydroxyurea is an established treatment for ameliorating SCD and improving life expectancy [1621,1692]. For patients with recurrent priapism, there is limited evidence to suggest a prophylactic role of hydroxyurea (LE: 3), [1679,1691,1693]. Adverse effects include oligo-zoospermia and leg ulcers.
10.2.1.4.8. Phosphodiesterase type 5 inhibitors
Low doses of PDE5Is have a paradoxical effect in alleviating and preventing stuttering priapism; mainly in patients with idiopathic and SCD-associated priapism [1573,1607,1668,1694-1698] (LE: 3). It is important to remember that therapy should be started when the penis is in its flaccid state and not during an acute episode. There is a delay of one week before treatment is effective. There are no reported impairments in male sexual function (LE: 3). Phosphodiesterase type 5 inhibitor treatment of stuttering priapism is possibly mediated by an increase in the concentration of cGMP in the smooth muscle in an NO dysfunctional state. This can occur in priapism and may result in a change in the NO pathway, with down-regulation of cavernosal PDE5 thereby preventing the complete degradation of cGMP in the corpus cavernosum [1573,1607,1668,1694].
10.2.1.4.9. Intracavernosal injections
Some patients with stuttering priapism, who have been started on systemic treatment to prevent recurrence of unwanted erections, may not see therapeutic benefits immediately and temporarily require intracavernous self-injections at home with sympathomimetic agents [1573,1607]. The most commonly used drugs are phenylephrine and etilephrine (as described in the treatment of ischaemic priapism) [1555,1593,1663,1677] (LE: 3). Adverse effects include hypertension, coronary ischaemia and cardiac arrhythmias.
Tissue plasminogen activator (TPA) is a secreted serine protease that converts the pro-enzyme plasminogen to plasmin, which acts as a fibrinolytic enzyme. Limited clinical data have suggested that a single intracavernous injection of TPA can successfully treat patients with recalcitrant priapism [1679,1699] (LE: 3). Mild bleeding is the most commonly observed adverse effect.
10.2.1.4.10. Penile prosthesis
Patients with medically refractory stuttering priapism require frequent visits to the emergency department and are always at risk of a major ischaemic episode, which can be mitigated with insertion of a penile prosthesis [1634,1654,1700]. Nevertheless, penile prosthesis for preventing stuttering priapism should not be offered before medical treatment and a penile prosthesis should be performed only in carefully selected patients as a last resort [1634]. In patients with permanent ED due to stuttering priapism, medical treatments for ED (PDE5Is or intracavernosal injection) should be used cautiously because of the risk of inducing an ischaemic episode and a penile prosthesis can be considered [1634,1701].
10.2.1.5. Summary of evidence for treatment of stuttering priapism
Summary of evidence | LE |
The primary goal in the management of patients with stuttering priapism is prevention of future episodes, which can generally be achieved pharmacologically. | 2b |
Phosphodiesterase type 5 inhibitors have a paradoxical effect in alleviating and preventing stuttering priapism, mainly in patients with idiopathic and SCD-associated priapism. | 3 |
The evidence with other systemic drugs (digoxin, α-adrenergic agonists, baclofen, gabapentin and terbutaline, hydroxyurea) is limited. | 3 |
10.2.1.6. Recommendations for treatment of stuttering priapism
Recommendations | Strength rating |
Manage each acute episode similar to that for ischaemic priapism. | Strong |
Use hormonal therapies (mainly gonadotropin-receptor hormone agonists or antagonists) and/or anti-androgens for the prevention of future episodes in patients with frequent relapses. Do not use them before sexual maturation is reached. | Weak |
Initiate treatment with phosphodiesterase type 5 inhibitors only when the penis is in its flaccid state. | Weak |
Use digoxin, α-adrenergic agonists, baclofen, gabapentin or terbutaline only in patients with frequent and uncontrolled relapses. | Weak |
Use intracavernous self-injections of sympathomimetic drugs at home for treatment of acute episodes on an interim basis until ischaemic priapism has been alleviated. | Weak |
10.2.1.7. Follow-up
Follow-up for stuttering priapism includes history and clinical examination to assess the efficacy of treatment in preventing or alleviating erectile events as well as assessing erectile function and penile fibrosis.
10.2.2. Priapism in children
The classification of priapism in children is similar to that in adults. In addition to ischaemic, stuttering and non-ischaemic priapism, a fourth type, neonatal priapism is also described [1555]. Priapism in children is considered rare as no data on its prevalence exist. Sickle cell disease is the major cause of priapism in children, followed by leukaemia (10%), trauma (10%), idiopathic causes (19%) and drugs (5%) [1702]. One study showed that 25% of children experienced SCD-related priapism in a pre-pubertal period [1703]. Another study revealed that 90% of men with SCD had their first priapism episode before age 20 years [1665]. Priapism in children should be evaluated and treated in a timely manner, as untreated ischaemic priapism may lead to ED and psychosexual disorders in adulthood [1704]. A multi-disciplinary team approach should be utilised with specialist input from haematologists and paediatric endocrinologists.
10.3. Non-ischaemic (high-flow or arterial) priapism
Most of the identified studies were small retrospective case series reporting principally on the role of embolisation in post-traumatic non-ischaemic priapism (Appendix 5). This may reflect the uncommon nature of the condition. Success rates and erectile function were well documented across all reports. Some studies attempted to stratify outcomes based on the agent used for embolisation (e.g., microcoil or autologous clot), although care should be taken when interpreting case series with small patient numbers.
10.3.1. Epidemiology/aetiology/pathophysiology
Epidemiological data on non-ischaemic priapism are almost exclusively derived from small case series [1555,1587,1589,1705,1706]. Non-ischaemic priapism is significantly less common than the ischaemic type, comprising only 5% of all priapism cases [1555]. The most frequent cause of non-ischaemic priapism is blunt perineal or penile trauma [1707]. The injury results in a laceration in the cavernosal artery or branches, leading to a fistula between the artery and the lacunar spaces of the sinusoidal space [1706]. The resultant increased blood flow results in a persistent and prolonged erection [1708].
There is often a delay between the trauma and the development of the priapism that may be up to two to three weeks [1709]. This is suggested to reflect either spasm or ischaemic necrosis of the injured artery, with the fistula only developing as the spasm resolves or when the ischaemic segment “blows up”. The priapism typically occurs after a nocturnal erection or an erection related to sexual activity, resulting in the sudden increase of blood flow and pressure in the cavernous arteries [1710]. The patient typically reports an erection that is not fully rigid and is not associated with pain because the venous drainage is not compromised and the penile tissue does not become ischaemic [1711].
Non-ischaemic priapism can occur after acute spinal cord injury, presumably due to loss of sympathetic input, leading to predominant parasympathetic input and increased arterial flow [1712]. It has also been reported to occur following internal urethrotomy [1713], Nesbit procedure [1714], circumcision [1715], transrectal prostate biopsy [1716], and brachytherapy for prostate cancer [1717]. Some cases have also been described following shunting procedures performed for ischaemic priapism due to a lacerated cavernosal artery (conversion of low-flow to high-flow priapism) [1718-1720]. Although SCD is usually associated with ischaemic priapism, occasional cases of high-flow priapism have been reported; however, the pathophysiological mechanism remains unclear [1721]. Finally, metastatic malignancy to the penis can also rarely cause non-ischaemic priapism [1722,1723] (Table 51).
Table 51: Causes of arterial priapism
Perineal or penile trauma |
Spinal cord injury |
Iatrogenic causes (e.g., shunting procedure for ischaemic priapism) |
Sickle cell disease |
Metastatic malignancy to the penis |
Idiopathic |
10.3.1.1. Summary of evidence on the epidemiology, aetiology and pathophysiology of arterial priapism
Summary of evidence | LE |
Non-ischaemic priapism is significantly less common than ischaemic priapism. | 2b |
Non-ischaemic priapism usually occurs after blunt perineal or penile trauma. | 2 |
Non-ischaemic priapism if not treated may cause erectile dysfunction with time. | 3 |
10.3.2. Classification
Non-ischaemic priapism is a persistent erection caused by unregulated cavernous arterial inflow [1555]. According to aetiology, non-ischaemic priapism can be categorised into four types: traumatic, neurogenic, iatrogenic and idiopathic in origin.
10.3.3. Diagnostic evaluation
10.3.3.1. History
A comprehensive history is mandatory in non-ischaemic priapism diagnosis and follows the same principles as described in Table 47. Arterial priapism should be suspected when the patient reports a history of pelvic, perineal, or genital trauma; no penile pain (discomfort is possible); and a persistent, not fully rigid erection (Table 48). The corpus cavernosum can become fully rigid with sexual stimulation, so the sexual intercourse is usually not compromised. The onset of post-traumatic non-ischaemic priapism can be delayed by several hours to weeks following the initial injury [1555].
10.3.3.2. Physical examination
In non-ischaemic priapism, the corpora are tumescent but not fully rigid. Abdominal, penile and perineal examination may reveal evidence of trauma (Table 46) [1555]. Neurological examination is indicated if a neurogenic aetiology is suspected.
10.3.3.3. Laboratory testing
Laboratory testing should include a blood count with white blood cell differential and a coagulation profile to assess for anaemia and other haematological abnormalities. Blood aspiration from the corpus cavernosum shows bright red arterial blood in arterial priapism, while blood is dark in ischaemic priapism (Table 47) (LE: 2b). Blood gas analysis is essential to differentiate between non-ischaemic and ischaemic priapism. Blood gas values in high-flow priapism show normal arterial blood [1555] (Table 48).
10.3.3.4. Penile imaging
Colour duplex US of the penis and perineum is recommended and can differentiate non-ischaemic from ischaemic priapism [1585-1587]. Ultrasound must be performed without intracavernosal vasoactive drug injection [1724]. In non-ischaemic priapism, US helps to localise the fistula site and appears as a characteristic colour blush and turbulent high-velocity flow on Doppler analysis [1725]. Patients with non-ischaemic priapism have normal to high blood velocities in the cavernous arteries [1556,1726].
Selective pudendal arteriography can reveal a characteristic blush at the site of injury in arterial priapism [1727,1728]. However, due to its invasiveness, it should be reserved for the management of non-ischaemic priapism when embolisation is being considered [1555,1581].
The role of MRI in the diagnostic evaluation of priapism is controversial. Its role in non-ischaemic priapism is limited because the small penile vessels and fistulae cannot be easily demonstrated [1729].
10.3.3.5. Recommendations for the diagnosis of non-ischaemic priapism
Recommendations | Strength rating |
Take a comprehensive history to establish the diagnosis, which can help to determine the priapism subtype. | Strong |
Include a physical examination of the genitalia, perineum and abdomen in the diagnostic evaluation. | Strong |
Include a neurological examination if neurogenic non-ischaemic priapism is suspected. | Strong |
For laboratory testing, include complete blood count, with white blood cell differential, and coagulation profile. | Strong |
Analyse the blood gas parameters from blood aspirated from the penis to differentiate between ischaemic and non-ischaemic priapism. | Strong |
Perform colour duplex ultrasound of the penis and perineum to differentiate between ischaemic and non-ischaemic priapism. | Strong |
Perform selected pudendal arteriography when embolisation is planned for non-ischaemic priapism. | Strong |
10.3.4. Disease management
Although the conventional belief is that the management of non-ischaemic priapism is not an emergency because the corpus cavernosum does not contain ischaemic blood, recent data indicate that the duration of non-ischaemic priapism can also impact erectile function. High-flow priapism was reproduced in an in vitro model using pre-contracted strips of rabbit corpus cavernosum superfused at high pO2 levels. This showed that the smooth muscle tone reduced by 43% after super-fusion for twelve hours, indicating irreversible smooth muscle dysfunction [1730]. In a case series consisting of six patients with high-flow priapism after median follow-up of 4.5 (2-12) weeks, all patients reported development of ED or distal penile flaccidity [1655]. The goal of treatment is closure of the fistula. Non-ischaemic priapism can be managed conservatively or by direct perineal compression. Failure of conservative treatment requires selective arterial embolisation [1731]. The optimal time interval between conservative treatment and arterial embolisation is still under debate. Definitive management can be performed at the discretion of the treating physician and should be discussed with the patients so that they can understand the risks of treatment [1555,1581].
10.3.4.1. Conservative management
Conservative management may include applying ice to the perineum or perineal compression, which is typically US-guided. The fistula occasionally closes spontaneously. Even in those cases where the fistula remains patent, intercourse is still possible [1587,1705,1732,1733]. Androgen deprivation therapy (e.g., leuprolide injections, bicalutamide and ketoconazole) has been reported in case series to enable closure of the fistula reducing spontaneous and sleep-related erections [1734]. However, sexual dysfunction due to these treatments must be considered. Patients may develop ED or distal penile flaccidity while undergoing conservative treatment [1655].
Blood aspiration is not helpful for the treatment of arterial priapism and the use of α-adrenergic antagonists is not recommended because of potential severe adverse effects (e.g., such as transfer of the drug into the systemic circulation).
10.3.4.2. Selective arterial embolisation
Selective arterial embolisation can be performed using temporary substances, such as autologous blood clot [1735-1737] and gel foam [1736,1738], or permanent substances such as microcoils [1736,1738-1740], ethylene-vinyl alcohol copolymer (PVA), and N-butyl-cyanoacrylate (NBCA) [1741]. It is assumed that temporary embolisation provides a decreased risk of ED, with the disadvantage of higher failure/recurrence rates; this would be the consequence of artery recanalisation using temporary materials. However, there is insufficient evidence to support this hypothesis. A recent non-systematic review of the literature reported success rates ranging between 61.7 and 83.3%, and ED rates from 0-33.3% after the first arterial embolisation, showing that failure/recurrence may not be significantly higher with temporary embolisation materials, and preservation of erectile function may not be that different between the two modalities either [1710]. Other potential complications of arterial embolisation include penile gangrene, gluteal ischaemia, cavernositis, and perineal abscess [1555,1742]. Repeated embolisation is a reasonable option for treating non-ischaemic priapism, both in terms of efficacy and safety [1710].
10.3.4.3. Surgical management
Surgical ligation of the fistula is possible through a transcorporeal or inguinoscrotal approach, using intra-operative Doppler US. Surgery is technically challenging and associated with significant risks, particularly of ED [1743]. Surgery is rarely performed and should only be considered when there are contraindications for selective embolisation, if embolisation is unavailable, or repeated embolisations have failed. If the patient desires more definitive treatment and is not sexually active or has pre-existing ED, surgical intervention can be an appropriate option [1710]. Erectile dysfunction rates ranging from 0-50% are reported following non-ischaemic priapism and its treatment, with surgical ligation having the highest reported rates [1710]. Patients can require penile prosthesis implantation for ED in the long-term [1634].
10.3.4.4. Summary of evidence for the treatment of arterial priapism
Summary of evidence | LE |
Non-ischaemic priapism can cause erectile dysfunction over time and early definitive management should be undertaken. | 3 |
Conservative management applying ice to the perineum or site-specific perineal compression is an option in all cases. The use of androgen deprivation therapy may enable closure of the fistula reducing spontaneous and sleep-related erections. | 3 |
Selective artery embolisation, using temporary or permanent substances, has high success rates. No definitive statement can be made on the best substance for embolisation in terms of sexual function preservation and success rate. | 3 |
Repeated embolisation is a reasonable option for the treatment of non-ischaemic priapism. | 2b |
Selective surgical ligation of the fistula should be reserved as the last treatment option when multiple embolisations have failed. | 3 |
10.3.4.5. Recommendations for the treatment of arterial priapism
Recommendations | Strength rating |
As non-ischaemic priapism is not an emergency, perform definitive management at the discretion of the treating physician. | Weak |
Manage conservatively with the use of site-specific perineal compression as the first step. Consider androgen deprivation therapy only in adults. | Weak |
Perform selective arterial embolisation when conservative management has failed. | Strong |
Perform first selective arterial embolisation using temporary material. | Weak |
Repeat the procedure with temporary or permanent material for recurrent non-ischaemic priapism following selective arterial embolisation. | Weak |
Reserve selective surgical ligation of a fistula as a final treatment option when repeated arterial embolisations have failed. | Weak |
10.3.4.6. High-flow priapism in children
Non-ischaemic priapism is a rare condition, especially in children. The embarrassment that children may have in speaking about it to their parents can lead to misdiagnosis and underestimating the prevalence of this condition [1744]. The aetiology, clinical presentation and diagnostic and therapeutic principles are comparable with those of arterial priapism in adults. However, some differentiating features should be noted.
Idiopathic non-ischaemic priapism can be found in a significant percentage of children [1745]. Perineal compression with the thumb may be a useful manoeuvre to distinguish ischaemic and non-ischaemic priapism, particularly in children, where it may result in immediate detumescence, followed by the return of the erection with the removal of compression [1710]. Conservative management using ice applied to the perineum or site-specific perineal compression may be successful, particularly in children [1746,1747]. Although reportedly successful, embolisation in children is technically challenging and requires treatment within a specialist paediatric vascular radiology department [1597,1748].
10.3.4.7. Follow-up
During conservative management of non-ischaemic priapism, physical examination and colour duplex US can be useful tools to assess treatment efficacy. Close follow-up using colour duplex US and MRI can help detect distal penile fibrosis and be beneficial in clinical decision-making to intervene with embolisation earlier [1655]. Follow-up after selective arterial embolisation should include clinical examination, colour duplex US, and erectile function assessment. If in doubt, repeat arteriography is required. The goals are to determine if the treatment was successful, identify signs of recurrence, and verify any anatomical and functional sequelae [1724].
10.4. Controversies and future areas of focus in the management of priapism
Low-flow priapism should be considered as a surgical emergency. Although the treatment of high-flow priapism can be delayed, there is some evidence to suggest that a delay in intervention may result in long-term fibrosis of the corpus cavernosum.
The evidence in the literature mainly consists of retrospective single centre cohort studies and therefore is of low quality. Prospective multicentre studies are needed to develop high levels of evidence to support contemporary guidelines.
There are a number of controversial areas including the prophylaxis of stuttering priapism, with no real evidence suggesting the superiority of a single pharmaceutical agent over another. In particular, understanding of the time point at which irreversible corporal smooth muscle necrosis occurs due to low-flow priapism is limited; therefore, definitive management of delayed or refractory priapism remains controversial (i.e., immediate prosthesis implantation vs. penoscrotal decompression vs. shunting). Therefore, it is strongly recommended that multi-centre collaborative studies are performed to better understand this rare but devastating condition.